
Page 649 - Cardiac Nursing
P. 649
CHAPTER 26 / Mechanical Circulatory Assist Devices 625
DISPLAY 26-2 Physiologic Effects and Expected Clinical
Outcomes of Balloon Inflation
Physiologic effects
Increased early diastolic pressure (by about 30%)
Diastolic augmentation
Increased aortic root pressure
Enhanced coronary artery perfusion pressure
Improved oxygen delivery
Decreased ischemia
Clinical outcomes
Early diastolic pressure $ systolic pressure
Decreased angina
Decreased signs of ischemia on the electrocardiogram
Decreased ventricular ectopy of ischemic origin
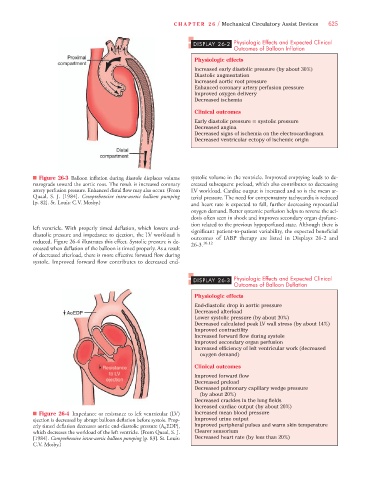
n Figure 26-3 Balloon inflation during diastole displaces volume systolic volume in the ventricle. Improved emptying leads to de-
retrograde toward the aortic root. The result is increased coronary creased subsequent preload, which also contributes to decreasing
artery perfusion pressure. Enhanced distal flow may also occur. (From LV workload. Cardiac output is increased and so is the mean ar-
Quaal, S. J. [1984]. Comprehensive intra-aortic balloon pumping terial pressure. The need for compensatory tachycardia is reduced
[p. 82]. St. Louis: C.V. Mosby.) and heart rate is expected to fall, further decreasing myocardial
oxygen demand. Better systemic perfusion helps to reverse the aci-
dosis often seen in shock and improves secondary organ dysfunc-
tion related to the previous hypoperfused state. Although there is
left ventricle. With properly timed deflation, which lowers end- significant patient-to-patient variability, the expected beneficial
diastolic pressure and impedance to ejection, the LV workload is outcomes of IABP therapy are listed in Displays 26-2 and
reduced. Figure 26-4 illustrates this effect. Systolic pressure is de- 26-3. 10,12
creased when deflation of the balloon is timed properly. As a result
of decreased afterload, there is more effective forward flow during
systole. Improved forward flow contributes to decreased end-
DISPLAY 26-3 Physiologic Effects and Expected Clinical
Outcomes of Balloon Deflation
Physiologic effects
End-diastolic drop in aortic pressure
Decreased afterload
Lower systolic pressure (by about 20%)
Decreased calculated peak LV wall stress (by about 14%)
Improved contractility
Increased forward flow during systole
Improved secondary organ perfusion
Increased efficiency of left ventricular work (decreased
oxygen demand)
Clinical outcomes
Improved forward flow
Decreased preload
Decreased pulmonary capillary wedge pressure
(by about 20%)
Decreased crackles in the lung fields
Increased cardiac output (by about 20%)
n Figure 26-4 Impedance or resistance to left ventricular (LV) Increased mean blood pressure
ejection is decreased by abrupt balloon deflation before systole. Prop- Improved urine output
erly timed deflation decreases aortic end-diastolic pressure (A 0 EDP), Improved peripheral pulses and warm skin temperature
which decreases the workload of the left ventricle. (From Quaal, S. J. Clearer sensorium
[1984]. Comprehensive intra-aortic balloon pumping [p. 83]. St. Louis: Decreased heart rate (by less than 20%)
C.V. Mosby.)