
Page 656 - Cardiac Nursing
P. 656
632 P AR T IV / Pathophysiology and Management of Heart Disease
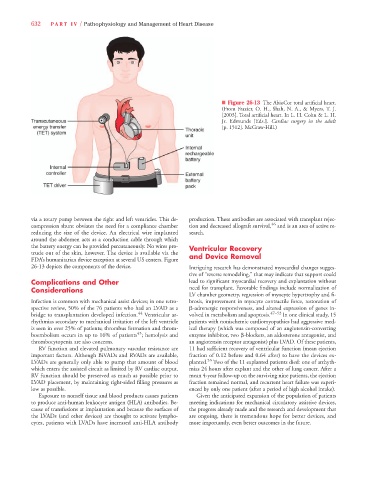
n Figure 26-13 The AbioCor total artificial heart.
(From Frazier, O. H., Shah, N. A., & Myers, T. J.
[2003]. Total artificial heart. In L. H. Cohn & L. H.
Jr. Edmunds [Eds.]. Cardiac surgery in the adult
[p. 1512]. McGraw-Hill.)
via a rotary pump between the right and left ventricles. This de- production. These antibodies are associated with transplant rejec-
compression shunt obviates the need for a compliance chamber tion and decreased allograft survival, 46 and is an area of active re-
reducing the size of the device. An electrical wire implanted search.
around the abdomen acts as a conduction cable through which
the battery energy can be provided percutaneously. No wires pro- Ventricular Recovery
trude out of the skin, however. The device is available via the and Device Removal
FDA’s humanitarian device exception at several US centers. Figure
26-13 depicts the components of the device. Intriguing research has demonstrated myocardial changes sugges-
tive of “reverse remodeling,” that may indicate that support could
Complications and Other lead to significant myocardial recovery and explantation without
Considerations need for transplant. Favorable findings include normalization of
LV chamber geometry, regression of myocyte hypertrophy and fi-
Infection is common with mechanical assist devices; in one retro- brosis, improvement in myocyte contractile force, restoration of
spective review, 50% of the 76 patients who had an LVAD as a b-adrenergic responsiveness, and altered expression of genes in-
bridge to transplantation developed infection. 44 Ventricular ar- volved in metabolism and apoptosis. 47–52 In one clinical study, 15
rhythmias secondary to mechanical irritation of the left ventricle patients with nonischemic cardiomyopathies had aggressive med-
is seen in over 25% of patients; thrombus formation and throm- ical therapy (which was composed of an angiotensin-converting
45
boembolism occurs in up to 16% of patients ; hemolysis and enzyme inhibitor, two b-blockers, an aldosterone antagonist, and
thrombocytopenia are also concerns. an angiotensin receptor antagonist) plus LVAD. Of these patients,
RV function and elevated pulmonary vascular resistance are 11 had sufficient recovery of ventricular function (mean ejection
important factors. Although BiVADs and RVADs are available, fraction of 0.12 before and 0.64 after) to have the devices ex-
53
LVADs are generally only able to pump that amount of blood planted. Two of the 11 explanted patients died: one of arrhyth-
which enters the assisted circuit as limited by RV cardiac output. mias 24 hours after explant and the other of lung cancer. After a
RV function should be preserved as much as possible prior to mean 4-year follow-up on the surviving nine patients, the ejection
LVAD placement, by maintaining right-sided filling pressures as fraction remained normal, and recurrent heart failure was experi-
low as possible. enced by only one patient (after a period of high alcohol intake).
Exposure to nonself tissue and blood products causes patients Given the anticipated expansion of the population of patients
to produce anti-human leukocyte antigen (HLA) antibodies. Be- meeting indications for mechanical circulatory assistive devices,
cause of transfusions at implantation and because the surfaces of the progress already made and the research and development that
the LVADs (and other devices) are thought to activate lympho- are ongoing, there is tremendous hope for better devices, and
cytes, patients with LVADs have increased anti-HLA antibody more importantly, even better outcomes in the future.