
Page 740 - Cardiac Nursing
P. 740
M
M
4 A
2:0
4 A
g
g
Pa
Pa
Pa
/09
/09
/30
6
/30
1
2:0
1
/09
1
g
ara
a
ara
t
t
c.
c.
In
a
In
16
16
16
e 7
e 7
p
p
p
A
A
LWB K34 0-c 29_ p p pp705-721.qxd 6/30/09 12:04 AM Page 716 Aptara Inc.
LWB
70
70
LWBK340-c29_
29_
29_
K34
0-c
5-7
q
q
xd
6
xd
21.
5-7
q
21.
716 PA R T I V / Pathophysiology and Management of Heart Disease
Physical Assessment TEE provides a more detailed look at the mitral valve and chordal
structures. 12
The classic auscultatory finding of MVP is a midsystolic click Cardiac catheterization can be used to rule out CHD as the
with mid- to late systolic murmur (see Table 29-3). The murmur origin of chest pain. Left ventriculography can demonstrate ab-
occurs secondary to regurgitant flow when the mitral valve leaflets normal motion of the mitral valve and help determine the degree
fail to approximate. Patients with MVP may have the murmur or of regurgitation.
click or both. Findings may also vary over time. When the degree Electrocardiography is nondiagnostic. The electrocardiogram
of mitral regurgitation is mild-to-moderate or less, heart rate and may be normal or have nonspecific ST-T-wave changes in the in-
blood pressure may be normal. Additional physical findings may ferior leads (II, III, and aVF) and occasionally in the anterolateral
include thin body habitus, pectus excavatum, straight back syn- leads (V 4 through V 6 ). The ST-T-wave changes may become more
V
drome, and scoliosis. notable with exercise. Premature atrial and ventricular complexes
may also be identified. Exercise testing may be used to help rule out
Diagnostic Tests the cause of the chest pain.
Chest radiography is often normal and is usually nondiagnostic
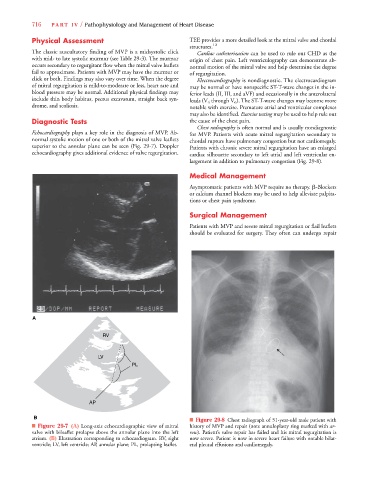
Echocardiography plays a key role in the diagnosis of MVP. Ab- for MVP. Patients with acute mitral regurgitation secondary to
normal systolic motion of one or both of the mitral valve leaflets chordal rupture have pulmonary congestion but not cardiomegaly.
superior to the annular plane can be seen (Fig. 29-7). Doppler Patients with chronic severe mitral regurgitation have an enlarged
echocardiography gives additional evidence of valve regurgitation. cardiac silhouette secondary to left atrial and left ventricular en-
largement in addition to pulmonary congestion (Fig. 29-8).
Medical Management
Asymptomatic patients with MVP require no therapy. -Blockers
or calcium channel blockers may be used to help alleviate palpita-
tions or chest pain syndrome.
Surgical Management
Patients with MVP and severe mitral regurgitation or flail leaflets
should be evaluated for surgery. They often can undergo repair
A
LV
PL
AP
B
■ Figure 29-8 Chest radiograph of 51-year-old male patient with
■ Figure 29-7 (A) Long-axis echocardiographic view of mitral history of MVP and repair (note annuloplasty ring marked with ar-
valve with bileaflet prolapse above the annular plane into the left row). Patient’s valve repair has failed and his mitral regurgitation is
atrium. (B) Illustration corresponding to echocardiogram. RV, right now severe. Patient is now in severe heart failure with notable bilat-
ventricle; LV, left ventricle; AP, annular plane; PL, prolapsing leaflet. eral pleural effusions and cardiomegaly.