
Page 309 - ACCCN's Critical Care Nursing
P. 309
286 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
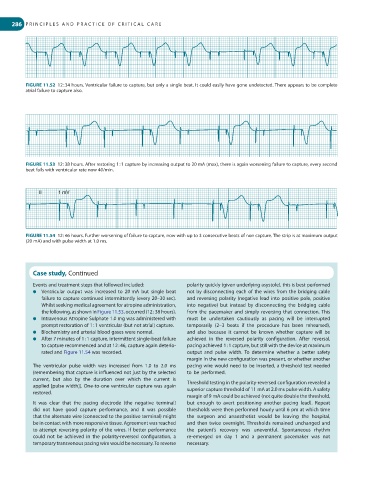
FIGURE 11.52 12 : 34 hours. Ventricular failure to capture, but only a single beat. It could easily have gone undetected. There appears to be complete
atrial failure to capture also.
FIGURE 11.53 12 : 38 hours. After restoring 1 : 1 capture by increasing output to 20 mA (max), there is again worsening failure to capture, every second
beat fails with ventricular rate now 40/min.
II 1 mV
FIGURE 11.54 12 : 46 hours. Further worsening of failure to capture, now with up to 3 consecutive beats of non capture. The strip is at maximum output
(20 mA) and with pulse width at 1.0 ms.
Case study, Continued
Events and treatment steps that followed included: polarity quickly (given underlying asystole), this is best performed
● Ventricular output was increased to 20 mA but single beat not by disconnecting each of the wires from the bridging cable
failure to capture continued intermittently (every 20–30 sec). and reversing polarity (negative lead into positive pole, positive
Whilst seeking medical agreement for atropine administration, into negative) but instead by disconnecting the bridging cable
the following, as shown in Figure 11.53, occurred (12 : 38 hours). from the pacemaker and simply reversing that connection. This
● Intravenous Atropine Sulphate 1.0 mg was administered with must be undertaken cautiously as pacing will be interrupted
prompt restoration of 1 : 1 ventricular (but not atrial) capture. temporarily (2–3 beats if the procedure has been rehearsed),
● Biochemistry and arterial blood gases were normal. and also because it cannot be known whether capture will be
● After 7 minutes of 1 : 1 capture, intermittent single-beat failure achieved in the reversed polarity configuration. After reversal,
to capture recommenced and at 12 : 46, capture again deterio- pacing achieved 1 : 1 capture, but still with the device at maximum
rated and Figure 11.54 was recorded. output and pulse width. To determine whether a better safety
margin in the new configuration was present, or whether another
The ventricular pulse width was increased from 1.0 to 2.0 ms pacing wire would need to be inserted, a threshold test needed
(remembering that capture is influenced not just by the selected to be performed.
current, but also by the duration over which the current is
applied [pulse width]). One-to-one ventricular capture was again Threshold testing in the polarity-reversed configuration revealed a
restored. superior capture threshold of 11 mA at 2.0 ms pulse width. A safety
margin of 9 mA could be achieved (not quite double the threshold,
It was clear that the pacing electrode (the negative terminal) but enough to avert positioning another pacing lead). Repeat
did not have good capture performance, and it was possible thresholds were then performed hourly until 6 pm at which time
that the alternate wire (connected to the positive terminal) might the surgeon and anaesthetist would be leaving the hospital,
be in contact with more responsive tissue. Agreement was reached and then twice overnight. Thresholds remained unchanged and
to attempt reversing polarity of the wires. If better performance the patient’s recovery was uneventful. Spontaneous rhythm
could not be achieved in the polarity-reversed configuration, a re-emerged on day 1 and a permanent pacemaker was not
temporary transvenous pacing wire would be necessary. To reverse necessary.