
Page 461 - ACCCN's Critical Care Nursing
P. 461
438 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
threshold in adults especially those who are pressure-
63
P1 active (i.e. ICP varies inversely with MAP). Higher CPP
P2 has been associated with increased lung water and acute
respiratory distress syndrome. Furthermore, mortality
P3
rises approximately 20% for each 10 mmHg loss of CPP.
In those studies where CPP was maintained above
70 mmHg, the reduction in mortality was as much as
64
35% for those with severe head injury. The Brain Trauma
Foundation recommends a CPP goal of 50–70 mmHg
A despite the lack of definitive data, such as from ran-
domised controlled trials and intention-to-treat clinical
65
P2 trials. In the paediatric population a CPP >40 mmHg is
the recommended guideline. 66,67 Utilising cerebral oxy-
P3 genation monitoring in combination with pressure has
been associated with better outcomes for brain-injured
P1 patients, and is part of the multimodal assessment for
brain injury.
ASSESSMENT OF CEREBRAL OXYGENATION
Jugular Venous Oximetry
B
Jugular venous catheterisation is used for deriving oxygen
68
based variables. It facilitates the assessment of jugular
venous oxygenation (SjvO 2 ), cerebral oxygen extraction
(CEO 2 ), and arteriovenous difference in oxygen (AVDO 2 ).
All of these variables indicate changes in cerebral metabo-
lism and blood flow, and therefore the catheter generates
continuous data that reflect the balance between supply
and demand of cerebral oxygen.
C
The catheter is inserted in the right jugular vein, as it is
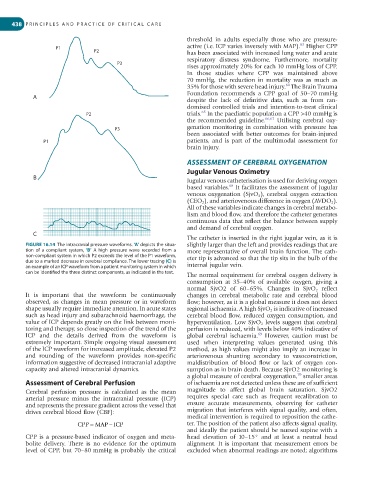
FIGURE 16.14 The intracranial pressure waveforms. ‘A’ depicts the situa- slightly larger than the left and provides readings that are
tion of a compliant system, ‘B’ A high pressure wave recorded from a more representative of overall brain function. The cath-
non-compliant system in which P2 exceeds the level of the P1 waveform, eter tip is advanced so that the tip sits in the bulb of the
due to a marked decrease in cerebral compliance. The lower tracing (C) is
an example of an ICP waveform from a patient monitoring system in which internal jugular vein.
can be identified the three distinct components, as indicated in the text.
The normal requirement for cerebral oxygen delivery is
consumption at 35–40% of available oxygen, giving a
normal SjvO2 of 60–65%. Changes in SjvO 2 reflect
It is important that the waveform be continuously changes in cerebral metabolic rate and cerebral blood
observed, as changes in mean pressure or in waveform flow; however, as it is a global measure it does not detect
shape usually require immediate attention. In acute states regional ischaemia. A high SjvO 2 is indicative of increased
such as head injury and subarachnoid haemorrhage, the cerebral blood flow, reduced oxygen consumption, and
value of ICP depends greatly on the link between moni- hyperventilation. Low SjvO 2 levels suggest that cerebral
toring and therapy, so close inspection of the trend of the perfusion is reduced, with levels below 40% indicative of
69
ICP and the details derived from the waveform is global cerebral ischaemia. However, caution must be
extremely important. Simple ongoing visual assessment used when interpreting values generated using this
of the ICP waveform for increased amplitude, elevated P2 method, as high values might also imply an increase in
and rounding of the waveform provides non-specific arteriovenous shunting secondary to vasoconstriction,
information suggestive of decreased intracranial adaptive maldistribution of blood flow or lack of oxygen con-
capacity and altered intracranial dynamics. sumption as in brain death. Because SjvO2 monitoring is
70
a global measure of cerebral oxygenation, smaller areas
Assessment of Cerebral Perfusion of ischaemia are not detected unless these are of sufficient
Cerebral perfusion pressure is calculated as the mean magnitude to affect global brain saturation. SjvO2
arterial pressure minus the intracranial pressure (ICP) requires special care such as frequent recalibration to
and represents the pressure gradient across the vessel that ensure accurate measurements, observing for catheter
drives cerebral blood flow (CBF): migration that interferes with signal quality, and often,
medical intervention is required to reposition the cathe-
−
CPP = MAP ICP ter. The position of the patient also affects signal quality,
and ideally the patient should be nursed supine with a
CPP is a pressure-based indicator of oxygen and meta- head elevation of 10–15° and at least a neutral head
bolite delivery. There is no evidence for the optimum alignment. It is important that measurement errors be
level of CPP, but 70–80 mmHg is probably the critical excluded when abnormal readings are noted; algorithms