
Page 470 - ACCCN's Critical Care Nursing
P. 470
Neurological Alterations and Management 447
Autonomic Nerve Dysfunction parenchyma. Accordingly, reduction of ICP is usually
Dysfunctions of the autonomic nervous system (ANS) argued for restoration of previously compromised cere-
or autonomic dysreflexia are recognised by the symptoms bral perfusion for improvement of cerebral metabolism.
that result from failure or imbalance of the sympathetic Although uncontrolled ICP elevation has been shown
or parasympathetic components of the ANS such as (i) to be responsible for reduced oxygen delivery, non-
increased (>120/min) or decreased (<50/min) heart rate, ischaemic impairment of oxidative metabolism and
(ii) increased respiratory rate (>24/min), (iii) raised mitochondrial damage has only recently been recog-
temperature (>38.5°C), (iv) increased (>160 mmHg) or nised as a prominent source of energy crisis triggered
decreased (<85 mmHg) systolic blood pressure, (v) by brain injury in the presence of adequate cerebral
12
increased muscle tone, (vi) decerebrate (extensor) or decor- blood flow. Accumulating evidence has shown that the
ticate (flexor) posturing, and (vii) profuse sweating. For mitochondrion has a pivotal role in post traumatic neu-
example, in spinal injury the presence of a noxious sti- ronal death by integrating numerous noxious signals
mulus can be transmitted from the periphery to the spinal responsible for both structural and functional damage
cord and activates dysfunctional sympathetic response. on one hand and by amplifying these signals through
activation of several cellular signalling events leading
There is strong evidence for numerous interactions among to cell death. In addition, more complex processes
the central nervous system (CNS), peripheral nervous with the alteration of cerebral perfusion, such as
system (both sympathetic and parasympathetic branches), cerebral hypoperfusion, ischaemia, reperfusion injury,
the endocrine system, and the immune system, hence inflammation and oedema result in increased intracra-
10
ANS dysfunction is related to that complex triad. Auto- nial pressure (ICP).
nomic nerve (AN) dysfunction ranges from alterations
in the sympathetic–parasympathetic balance to almost Cerebral Ischaemia
complete cessation as occurs in spinal cord injury. As the
ANS controls organ function AN dysfunction is related to Ischaemia is the inadequate delivery of oxygen, the inad-
all-organ alteration and failure. The immune system is equate removal of carbon dioxide from the cell, and an
connected to the nervous system through the ANS with increase in the production of intracellular lactic acid.
many of the patients with infections, systemic inflamma- Ischaemia can be caused by an increase in nutrient utilisa-
tory response and multi-organ failure exhibiting AN dys- tion by the brain in a hyperactive state, a decrease in
function. AN dysfunction is closely related to systemic delivery related to either cerebral or systemic complica-
13
inflammation hence those with conditions with increased tions, and/or a mismatch between delivery and demand.
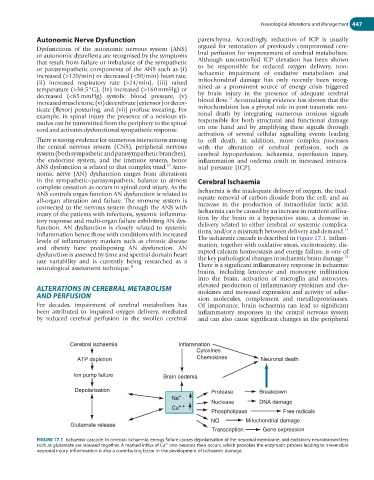
levels of inflammatory markers such as chronic disease The ischaemic cascade is described in Figure 17.1. Inflam-
and obesity have predisposing AN dysfunction. AN mation, together with oxidative stress, excitotoxicity, dis-
dysfunction is assessed by time and spectral domain heart rupted calcium homeostasis and energy failure, is one of
14
rate variability and is currently being researched as a the key pathological changes in ischaemic brain damage.
neurological assessment technique. 11 There is a significant inflammatory response in ischaemic
brains, including leucocyte and monocyte infiltration
into the brain, activation of microglia and astrocytes,
ALTERATIONS IN CEREBRAL METABOLISM elevated production of inflammatory cytokines and che-
mokines and increased expression and activity of adhe-
AND PERFUSION sion molecules, complement and metalloproteinases.
For decades, impairment of cerebral metabolism has Of importance, brain ischaemia can lead to significant
been attributed to impaired oxygen delivery, mediated inflammatory responses in the central nervous system
by reduced cerebral perfusion in the swollen cerebral and can also cause significant changes in the peripheral
Cerebral ischaemia Inflammation
Cytokines
ATP depletion Chemokines Neuronal death
Ion pump failure Brain oedema
Depolarisation Protease Breakdown
Na +
Nuclease DNA damage
Ca + +
Phospholipase Free radicals
NO Mitochondrial damage
Glutamate release
Transcription Gene expression
FIGURE 17.1 Ischaemic cascade. In cerebral ischaemia, energy failure causes depolarisation of the neuronal membrane, and excitatory neurotransmitters
such as glutamate are released together. A marked influx of Ca into neurons then occurs, which provokes the enzymatic process leading to irreversible
2+
neuronal injury. Inflammation is also a contributing factor in the development of ischaemic damage.