
Page 474 - ACCCN's Critical Care Nursing
P. 474
Neurological Alterations and Management 451
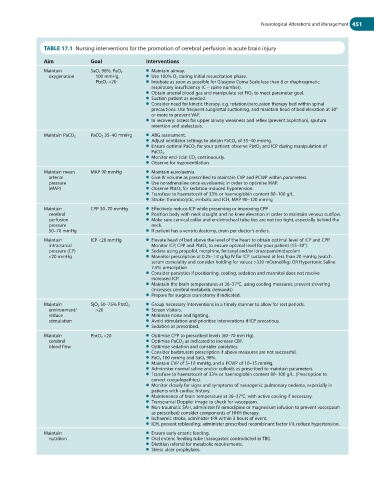
TABLE 17.1 Nursing interventions for the promotion of cerebral perfusion in acute brain injury
Aim Goal Interventions
Maintain SaO 2 98%, PaO 2 ● Maintain airway.
oxygenation 100 mmHg, ● Use 100% O 2 during initial resuscitation phase.
PbtO 2 >20 ● Intubate as soon as possible for Glasgow Coma Scale less than 8 or diaphragmatic
respiratory insufficiency (C – spine number).
● Obtain arterial blood gas and manipulate set FiO 2 to meet parameter goal.
● Suction patient as needed.
● Consider need for kinetic therapy, e.g. rotation/percussion therapy bed within spinal
precautions. Use frequent subglottal suctioning, and maintain head of bed elevation at 30°
or more to prevent VAP.
● In recovery: assess for upper airway weakness and reflex (prevent aspiration), sputum
retention and atelectasis.
PaCO 2 35–40 mmHg ● ABG assessment.
Maintain PaCO 2
● Adjust ventilator settings to obtain PaCO 2 of 35–40 mmHg.
● Ensure optimal PaCO 2 for your patient: observe PbtO 2 and ICP during manipulation of
PaCO 2 .
● Monitor end-tidal CO 2 continuously.
● Observe for hypoventilation.
Maintain mean MAP 90 mmHg ● Maintain euvolaemia.
arterial ● Give IV volume as prescribed to maintain CVP and PCWP within parameters.
pressure ● Use noradrenaline once euvolaemic in order to optimise MAP.
(MAP) ● Observe PbtO 2 for sedation-induced hypotension.
● Transfuse to haematocrit of 33% or haemoglobin content 80–100 g/L.
● Stroke: thrombolytic, embolic and ICH, MAP 90–120 mmHg
Maintain CPP 50–70 mmHg ● Effectively reduce ICP while preserving or improving CPP
cerebral ● Position body with neck straight and no knee elevation in order to maintain venous outflow.
perfusion ● Make sure cervical collar and endotracheal tube ties are not too tight, especially behind the
pressure neck.
50–70 mmHg ● If patient has a ventriculostomy, drain per doctor’s orders.
Maintain ICP <20 mmHg ● Elevate head of bed above the level of the heart to obtain optimal level of ICP and CPP.
intracranial Monitor ICP, CPP and PbtO 2 to ensure optimal level for your patient (15–30°).
pressure (CP) ● Sedate using propofol, morphine, fentanyl and/or lorazepam/midazolam
<20 mmHg ● Mannitol prescription at 0.25–1.0 g/kg IV for ICP sustained at less than 20 mmHg (watch
serum osmolality and consider holding for values >320 mOsmol/kg) OR Hypertonic Saline
7.5% prescription
● Consider paralytics if positioning, cooling, sedation and mannitol does not resolve
increased ICP.
● Maintain the brain temperatures at 36–37°C, using cooling measures; prevent shivering
(increases cerebral metabolic demands)
● Prepare for surgical craniotomy if indicated.
Maintain SjO 2 50–75% PbtO 2 ● Group necessary interventions in a timely manner to allow for rest periods.
environment/ >20 ● Screen visitors.
reduce ● Minimise noise and lighting.
stimulation ● Avoid stimulation and prioritise interventions if ICP precarious.
● Sedation as prescribed.
Maintain PbtO 2 <20 ● Optimise CPP to prescribed levels (60–70 mm Hg).
cerebral ● Optimise PaCO 2 as indicated to increase CBF.
blood flow ● Optimise sedation and consider paralytics.
● Consider barbiturate prescription if above measures are not successful.
● PaO 2 100 mmHg and SaO 2 98%.
● Maintain CVP of 5–10 mmHg, and a PCWP of 10–15 mmHg.
● Administer normal saline and/or colloids as prescribed to maintain parameters.
● Transfuse to haematocrit of 33% or haemoglobin content 80–100 g/L. (Prescription to
correct coagulopathies).
● Monitor closely for signs and symptoms of neurogenic pulmonary oedema, especially in
patients with cardiac history.
● Maintenance of brain temperature at 36–37°C, with active cooling if necessary.
● Transcranial Doppler image to check for vasospasm.
● Non-traumatic SAH, administer IV nimodipine or magnesium infusion to prevent vasospasm
as prescribed; consider components of HHH therapy.
● Ischaemic stroke, administer tPA within 3 hours of event.
● ICH, prevent rebleeding; administer prescribed recombinant factor VII, reduce hypertension.
Maintain ● Ensure early enteric feeding.
nutrition ● Oral enteric feeding tube (nasogastric contradicted in TBI).
● Dietitian referral for metabolic requirements.
● Stress ulcer prophylaxis.