
Page 472 - ACCCN's Critical Care Nursing
P. 472
Neurological Alterations and Management 449
Intracranial pressure (mmHg) 50 Cerebral blood flow (mL/min) 100 (partial pressure of
60
PaCO 2
40
carbon dioxide)
30
50
20
10
0
Volume (mL) 0 0 5 10 15
PaCO (kPa)
Relationship between ICP and intracranial volume 2
Relationship between CBF and PaCO 2
Cerebral blood flow (CBF) mL/min Cerebral blood flow (mL/min) 100 (partial pressure 2
PaO
50
50
of oxygen)
50 mmHg 150 mmHg 0 0 5 10 15
Mean arterial pressure (MAP) PaO (kPa)
2
Relationship between CBF and MAP Relationship between CBF and PaO 2
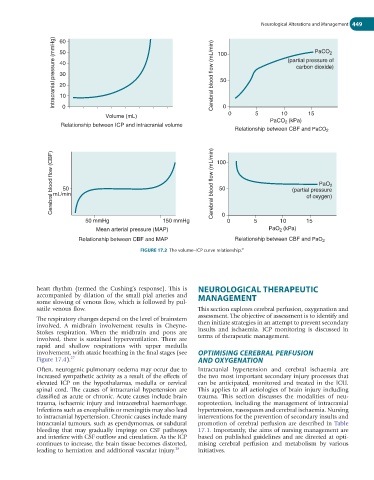
FIGURE 17.2 The volume–ICP curve relationship.
21
heart rhythm (termed the Cushing’s response). This is NEUROLOGICAL THERAPEUTIC
accompanied by dilation of the small pial arteries and MANAGEMENT
some slowing of venous flow, which is followed by pul-
satile venous flow. This section explores cerebral perfusion, oxygenation and
assessment. The objective of assessment is to identify and
The respiratory changes depend on the level of brainstem
involved. A midbrain involvement results in Cheyne- then initiate strategies in an attempt to prevent secondary
Stokes respiration. When the midbrain and pons are insults and ischaemia. ICP monitoring is discussed in
involved, there is sustained hyperventilation. There are terms of therapeutic management.
rapid and shallow respirations with upper medulla
involvement, with ataxic breathing in the final stages (see OPTIMISING CEREBRAL PERFUSION
Figure 17.4). 27 AND OXYGENATION
Often, neurogenic pulmonary oedema may occur due to Intracranial hypertension and cerebral ischaemia are
increased sympathetic activity as a result of the effects of the two most important secondary injury processes that
elevated ICP on the hypothalamus, medulla or cervical can be anticipated, monitored and treated in the ICU.
spinal cord. The causes of intracranial hypertension are This applies to all aetiologies of brain injury including
classified as acute or chronic. Acute causes include brain trauma. This section discusses the modalities of neu-
trauma, ischaemic injury and intracerebral haemorrhage. roprotection, including the management of intracranial
Infections such as encephalitis or meningitis may also lead hypertension, vasospasm and cerebral ischaemia. Nursing
to intracranial hypertension. Chronic causes include many interventions for the prevention of secondary insults and
intracranial tumours, such as ependymomas, or subdural promotion of cerebral perfusion are described in Table
bleeding that may gradually impinge on CSF pathways 17.1. Imp ortantly, the aims of nursing management are
and interfere with CSF outflow and circulation. As the ICP based on published guidelines and are directed at opti-
continues to increase, the brain tissue becomes distorted, mising cer ebral perfusion and metabolism by various
leading to herniation and additional vascular injury. 28 initiatives.