
Page 684 - ACCCN's Critical Care Nursing
P. 684
Resuscitation 661
Advanced Life Support
for Adults
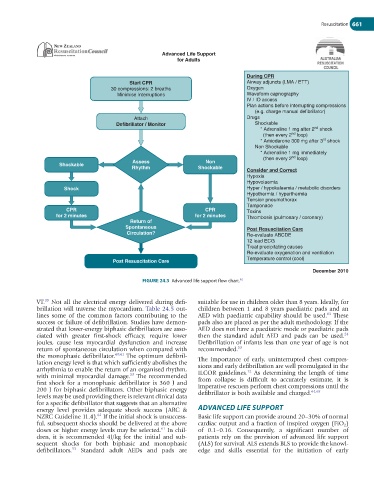
During CPR
Start CPR Airway adjuncts (LMA / ETT)
30 compressions: 2 breaths Oxygen
Minimise Interruptions Waveform capnography
IV / IO access
Plan actions before interrupting compressions
(e.g. charge manual defibrillator)
Attach Drugs
Defibrillator / Monitor Shockable
nd
* Adrenaline 1 mg after 2 shock
nd
(then every 2 loop)
rd
* Amiodarone 300 mg after 3 shock
Non Shockable
* Adrenaline 1 mg immediately
nd
(then every 2 loop)
Assess Non
Shockable
Rhythm Shockable
Consider and Correct
Hypoxia
Hypovolaemia
Shock Hyper / hypokalaemia / metabolic disorders
Hypothermia / hyperthermia
Tension pneumothorax
Tamponade
CPR CPR Toxins
for 2 minutes for 2 minutes Thrombosis (pulmonary / coronary)
Return of
Spontaneous Post Resuscitation Care
Circulation? Re-evaluate ABCDE
12 lead ECG
Treat precipitating causes
Re-evaluate oxygenation and ventilation
Temperature control (cool)
Post Resuscitation Care
December 2010
62
FIGURE 24.3 Advanced life support flow chart.
39
VT. Not all the electrical energy delivered during defi- suitable for use in children older than 8 years. Ideally, for
brillation will traverse the myocardium. Table 24.5 out- children between 1 and 8 years paediatric pads and an
63
lines some of the common factors contributing to the AED with paediatric capability should be used. These
success or failure of defibrillation. Studies have demon- pads also are placed as per the adult methodology. If the
strated that lower-energy biphasic defibrillators are asso- AED does not have a paediatric mode or paediatric pads
24
ciated with greater first-shock efficacy, require lower then the standard adult AED and pads can be used.
joules, cause less myocardial dysfunction and increase Defibrillation of infants less than one year of age is not
return of spontaneous circulation when compared with recommended. 53
the monophasic defibrillator. 60,61 The optimum defibril- The importance of early, uninterrupted chest compres-
lation energy level is that which sufficiently abolishes the sions and early defibrillation are well promulgated in the
arrhythmia to enable the return of an organised rhythm, ILCOR guidelines. As determining the length of time
12
53
with minimal myocardial damage. The recommended from collapse is difficult to accurately estimate, it is
first shock for a monophasic defibrillator is 360 J and imperative rescuers perform chest compressions until the
200 J for biphasic defibrillators. Other biphasic energy defibrillator is both available and charged. 64,65
levels may be used providing there is relevant clinical data
for a specific defibrillator that suggests that an alternative
energy level provides adequate shock success (ARC & ADVANCED LIFE SUPPORT
62
NZRC Guideline 11.4). If the initial shock is unsuccess- Basic life support can provide around 20–30% of normal
ful, subsequent shocks should be delivered at the above cardiac output and a fraction of inspired oxygen (FiO 2 )
61
doses or higher energy levels may be selected. In chil- of 0.1–0.16. Consequently, a significant number of
dren, it is recommended 4J/kg for the initial and sub- patients rely on the provision of advanced life support
sequent shocks for both biphasic and monophasic (ALS) for survival. ALS extends BLS to provide the knowl-
53
defibrillators. Standard adult AEDs and pads are edge and skills essential for the initiation of early