
Page 526 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 526
18 Female Genital System 511
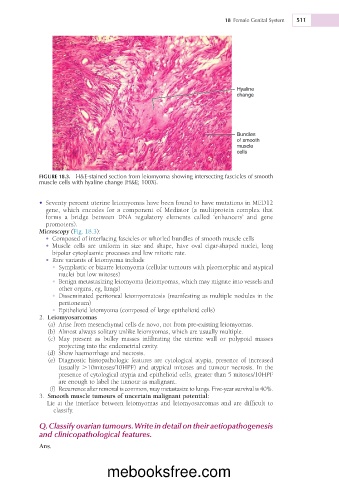
Hyaline
change
Bundles
of smooth
muscle
cells
FIGURE 18.3. H&E-stained section from leiomyoma showing intersecting fascicles of smooth
muscle cells with hyaline change (H&E; 100X).
• Seventy percent uterine leiomyomas have been found to have mutations in MED12
gene, which encodes for a component of Mediator (a multiprotein complex that
forms a bridge between DNA regulatory elements called ‘enhancers’ and gene
promoters).
Microscopy (Fig. 18.3):
• Composed of interlacing fascicles or whorled bundles of smooth muscle cells
• Muscle cells are uniform in size and shape, have oval cigar-shaped nuclei, long
bipolar cytoplasmic processes and low mitotic rate.
• Rare variants of leiomyoma include
• Symplastic or bizarre leiomyoma (cellular tumours with pleomorphic and atypical
nuclei but low mitoses)
• Benign metastasizing leiomyoma (leiomyomas, which may migrate into vessels and
other organs, eg, lungs)
• Disseminated peritoneal leiomyomatosis (manifesting as multiple nodules in the
peritoneum)
• Epithelioid leiomyoma (composed of large epithelioid cells)
2. Leiomyosarcomas
(a) Arise from mesenchymal cells de novo, not from pre-existing leiomyomas.
(b) Almost always solitary unlike leiomyomas, which are usually multiple.
(c) May present as bulky masses infiltrating the uterine wall or polypoid masses
projecting into the endometrial cavity.
(d) Show haemorrhage and necrosis.
(e) Diagnostic histopathologic features are cytological atypia, presence of increased
(usually .10mitoses/10HPF) and atypical mitoses and tumour necrosis. In the
presence of cytological atypia and epithelioid cells, greater than 5 mitoses/10HPF
are enough to label the tumour as malignant.
(f) Recurrence after removal is common, may metastasize to lungs. Five-year survival is 40%.
3. Smooth muscle tumours of uncertain malignant potential:
Lie at the interface between leiomyomas and leiomyosarcomas and are difficult to
classify.
Q. Classify ovarian tumours. Write in detail on their aetiopathogenesis
and clinicopathological features.
Ans.
mebooksfree.com