
Page 1621 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1621
1442 Part VII Hematologic Malignancies
response without a significant risk of recurrent amyloid when the CONCLUSIONS
primary hematologic disorder is controlled.
Nine cardiac transplants were reported from Boston, eight of Amyloidosis should always be considered in the differential diagnosis
whom subsequently received a stem cell transplant. Six of seven of a patient who presents with proteinuria and is nondiabetic. Any
evaluable patients achieved a complete hematologic remission. One patient with unexplained fatigue or restrictive cardiomyopathy or
achieved a partial remission. At a median follow-up of 56 months, heart failure with preserved ejection fraction should be screened for
five of seven patients were alive without recurrent amyloid, compa- amyloidosis. Patients who fulfill criteria for chronic inflammatory
rable to patients who received heart transplants for nonamyloid heart demyelinating peripheral neuropathy, unexplained hepatomegaly, or
disease. At Mayo Clinic, the median survival of patients who have atypical multiple myeloma should all be considered for the possibility
received cardiac transplants for amyloid is approximately 50%, which of amyloidosis. When a patient with one of these five compatible
is somewhat inferior to patients who receive hearts for cardiomyopa- syndromes is seen, screening with immunofixation of the serum or
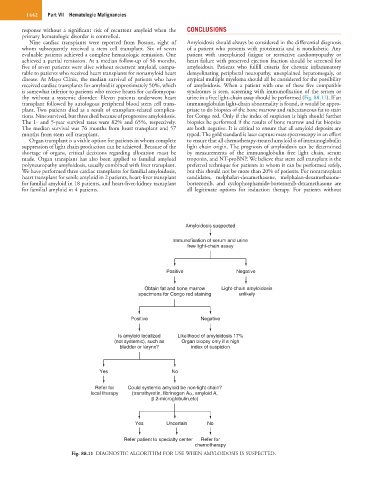
thy without a systemic disorder. Eleven patients underwent heart urine in a free light-chain assay should be performed (Fig. 88.11). If an
transplant followed by autologous peripheral blood stem cell trans- immunoglobulin light-chain abnormality is found, it would be appro-
plant. Two patients died as a result of transplant-related complica- priate to do biopsies of the bone marrow and subcutaneous fat to stain
tions. Nine survived, but three died because of progressive amyloidosis. for Congo red. Only if the index of suspicion is high should further
The 1- and 5-year survival rates were 82% and 65%, respectively. biopsies be performed if the results of bone marrow and fat biopsies
The median survival was 76 months from heart transplant and 57 are both negative. It is critical to ensure that all amyloid deposits are
months from stem cell transplant. typed. The gold standard is laser capture mass spectroscopy in an effort
Organ transplant is a viable option for patients in whom complete to ensure that all chemotherapy-treated amyloid is of immunoglobulin
suppression of light chain production can be achieved. Because of the light chain origin. The prognosis of amyloidosis can be determined
shortage of organs, critical decisions regarding allocation must be by measurements of the immunoglobulin free light chain, serum
made. Organ transplant has also been applied to familial amyloid troponin, and NT-proBNP. We believe that stem cell transplant is the
polyneuropathy amyloidosis, usually combined with liver transplant. preferred technique for patients in whom it can be performed safely,
We have performed three cardiac transplants for familial amyloidosis, but this should not be more than 20% of patients. For nontransplant
heart transplant for senile amyloid in 2 patients, heart-liver transplant candidates, melphalan-dexamethasone, melphalan-dexamethasone-
for familial amyloid in 18 patients, and heart-liver-kidney transplant bortezomib, and cyclophosphamide-bortezomib-dexamethasone are
for familial amyloid in 4 patients. all legitimate options for induction therapy. For patients without
Amyloidosis suspected
lmmunofixation of serum and urine
free light-chain assay
Positive Negative
Obtain fat and bone marrow Light-chain amyloidosis
specimens for Congo red staining unlikely
Positive Negative
Is amyloid localized Likelihood of amyloidosis 17%
(not systemic), such as Organ biopsy only if a high
bladder or larynx? index of suspicion
Yes No
Refer for Could systemic amyloid be non-light chain?
local therapy (transthyretin, fibrinogen A , amyloid A,
2-microglobulin,etc)
Yes Uncertain No
Refer patient to specialty center Refer for
chemotherapy
Fig. 88.11 DIAGNOSTIC ALGORITHM FOR USE WHEN AMYLOIDOSIS IS SUSPECTED.