
Page 842 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 842
Chapter 52 Histiocytic Disorders 725
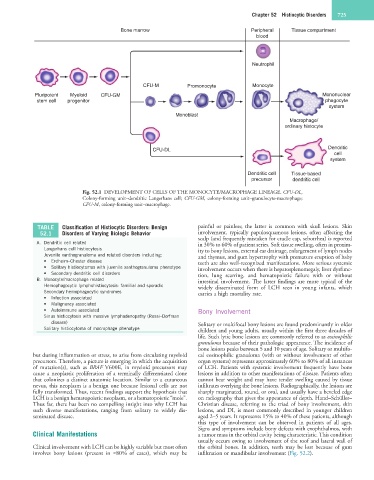
Bone marrow Peripheral Tissue compartment
blood
Neutrophil
CFU-M Promonocyte Monocyte
Pluripotent Myeloid CFU-GM Mononuclear
stem cell progenitor phagocyte
system
Monoblast
Macrophage/
ordinary histocyte
CFU-DL Dendritic
cell
system
Dendritic cell Tissue-based
precursor dendritic cell
Fig. 52.1 DEVELOPMENT OF CELLS OF THE MONOCYTE/MACROPHAGE LINEAGE. CFU-DL,
Colony-forming unit–dendritic Langerhans cell; CFU-GM, colony-forming unit–granulocyte-macrophage;
CFU-M, colony-forming unit–macrophage.
TABLE Classification of Histiocytic Disorders: Benign painful or painless; the latter is common with skull lesions. Skin
52.1 Disorders of Varying Biologic Behavior involvement, typically papulosquamous lesions, often affecting the
scalp (and frequently mistaken for cradle cap, seborrhea) is reported
A. Dendritic cell related in 30% to 60% of patient series. Soft tissue swelling, often in proxim-
Langerhans cell histiocytosis ity to bony lesions, external ear drainage, enlargement of lymph nodes
Juvenile xanthogranuloma and related disorders including: and thymus, and gum hypertrophy with premature eruption of baby
• Erdheim–Chester disease teeth are also well-recognized manifestations. More serious systemic
• Solitary histiocytomas with juvenile xanthogranuloma phenotype involvement occurs when there is hepatosplenomegaly, liver dysfunc-
• Secondary dendritic cell disorders tion, lung scarring, and hematopoietic failure with or without
B. Monocyte/macrophage related intestinal involvement. The latter findings are more typical of the
Hemophagocytic lymphohistiocytosis: familial and sporadic widely disseminated form of LCH seen in young infants, which
Secondary hemophagocytic syndromes carries a high mortality rate.
• Infection associated
• Malignancy associated
• Autoimmune associated Bony Involvement
Sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman
disease) Solitary or multifocal bony lesions are found predominantly in older
Solitary histiocytoma of macrophage phenotype children and young adults, usually within the first three decades of
life. Such lytic bone lesions are commonly referred to as eosinophilic
granuloma because of their pathologic appearance. The incidence of
bone lesions peaks between 5 and 10 years of age. Solitary or multifo-
but during inflammation or stress, to arise from circulating myeloid cal eosinophilic granuloma (with or without involvement of other
precursors. Therefore, a picture is emerging in which the acquisition organ systems) represents approximately 60% to 80% of all instances
of mutation(s), such as BRAF V600E, in myeloid precursors may of LCH. Patients with systemic involvement frequently have bone
cause a neoplastic proliferation of a terminally differentiated clone lesions in addition to other manifestations of disease. Patients often
that colonizes a distinct anatomic location. Similar to a cutaneous cannot bear weight and may have tender swelling caused by tissue
nevus, this neoplasm is a benign one because lesional cells are not infiltrates overlying the bone lesions. Radiographically, the lesions are
fully transformed. Thus, recent findings support the hypothesis that sharply marginated, round, or oval, and usually have a beveled edge
LCH is a benign hematopoietic neoplasm, or a hematopoietic “mole”. on radiography that gives the appearance of depth. Hand–Schüller–
Thus far, there has been no compelling insight into why LCH has Christian disease, referring to the triad of bony involvement, skin
such diverse manifestations, ranging from solitary to widely dis- lesions, and DI, is most commonly described in younger children
seminated disease. aged 2–5 years. It represents 15% to 40% of these patients, although
this type of involvement can be observed in patients of all ages.
Signs and symptoms include bony defects with exophthalmos, with
Clinical Manifestations a tumor mass in the orbital cavity being characteristic. This condition
usually occurs owing to involvement of the roof and lateral wall of
Clinical involvement with LCH can be highly variable but most often the orbital bones. In addition, teeth may be lost because of gum
involves bony lesions (present in ≈80% of cases), which may be infiltration or mandibular involvement (Fig. 52.2).