
Page 873 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 873
756 Part VI Non-Malignant Leukocytes
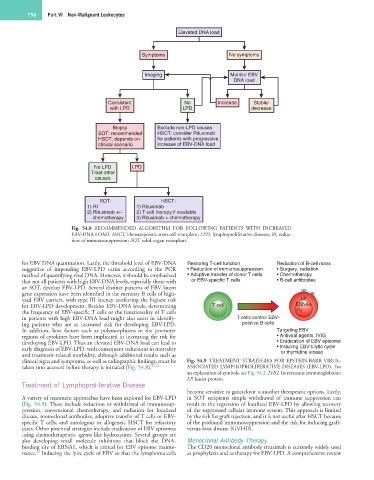
Elevated DNA load
Symptoms No symptoms
Imaging Monitor EBV
DNA load
Consistent No Increase Stable/
with LPD LPD decrease
Biopsy Exclude non-LPD causes
SOT: recommended HSCT: consider Rituximab
HSCT: depends on for patients with progressive
clinical scenario increase of EBV-DNA load
No LPD LPD
Treat other
causes
SOT: HSCT:
1) RI 1) Rituximab
2) Rituximab +/– 2) T-cell therapy if available
chemotherapy 3) Rituximab + chemotherapy
Fig. 54.8 RECOMMENDED ALGORITHM FOR FOLLOWING PATIENTS WITH INCREASED
EBV-DNA LOAD. HSCT, Hematopoietic stem cell transplant; LPD, lymphoproliferative diseases; RI, reduc-
tion of immunosuppression; SOT, solid organ transplant.
for EBV DNA quantitation. Lastly, the threshold level of EBV-DNA Restoring T-cell function Reduction of B-cell mass
suggestive of impending EBV-LPD varies according to the PCR • Reduction of immunosuppression • Surgery, radiation
method of quantifying viral DNA. However, it should be emphasized • Adoptive transfer of donor T cells • Chemotherapy
that not all patients with high EBV-DNA levels, especially those with or EBV-specific T cells • B-cell antibodies
an SOT, develop EBV-LPD. Several distinct patterns of EBV latent
gene expression have been identified in the memory B cells of high-
load EBV carriers, with type III latency conferring the highest risk LP
for EBV-LPD development. Besides EBV-DNA levels, determining T cell EBNAs
the frequency of EBV-specific T cells or the functionality of T cells
in patients with high EBV-DNA load might also assist in identify- T cells control EBV-
ing patients who are at increased risk for developing EBV-LPD. positive B cells
In addition, host factors such as polymorphisms in the promoter Targeting EBV
regions of cytokines have been implicated in increasing the risk for • Antiviral agents, IVIG
developing EBV-LPD. Thus an elevated EBV-DNA load can lead to • Eradication of EBV episome
early diagnosis of EBV-LPD, with consequent reductions in mortality • Inducing EBV’s lytic cycle
and treatment-related morbidity, although additional results such as or thymidine kinase
clinical signs and symptoms, as well as radiographic findings, must be Fig. 54.9 TREATMENT STRATEGIES FOR EPSTEIN-BARR VIRUS–
taken into account before therapy is initiated (Fig. 54.8). 21,22 ASSOCIATED LYMPHOPROLIFERATIVE DISEASES (EBV-LPD). For
an explanation of symbols, see Fig. 54.2. IVIG, Intravenous immunoglobulin;
LP, leader protein.
Treatment of Lymphoproliferative Disease
become sensitive to ganciclovir is another therapeutic options. Lastly,
A variety of treatment approaches have been explored for EBV-LPD in SOT recipients simple withdrawal of immune suppression can
(Fig. 54.9). These include reduction or withdrawal of immunosup- result in the regression of localized EBV-LPD by allowing recovery
pression, conventional chemotherapy, and radiation for localized of the suppressed cellular immune system. This approach is limited
disease, monoclonal antibodies, adoptive transfer of T cells or EBV- by the risk for graft rejection, and it is not useful after HSCT because
specific T cells, and autologous or allogeneic HSCT for refractory of the profound immunosuppression and the risk for inducing graft-
cases. Other potential strategies include eradication of EBV episomes versus-host disease (GVHD).
using chemotherapeutic agents like hydroxyurea. Several groups are
also developing small molecule inhibitors that block the DNA- Monoclonal Antibody Therapy
binding site of EBNA1, which is critical for EBV episome mainte- The CD20 monoclonal antibody rituximab is currently widely used
23
nance. Inducing the lytic cycle of EBV so that the lymphoma cells as prophylaxis and as therapy for EBV-LPD. A comprehensive review