
Page 2152 - Williams Hematology ( PDFDrive )
P. 2152
2126 Part XII: Hemostasis and Thrombosis Chapter 123: Hemophilia A and Hemophilia B 2127
Exons 1 2 3 4 5 6 7 8
Gene 5' 3' (35 kb)
mRNA
5' 3'
Exons 1 2 3 4 5 ∗ 6 ∗ 7 8
Sig/PP GLA EGF1 EGF2 Activation peptide Protease domain
1 145 180 415
Tyr Thr
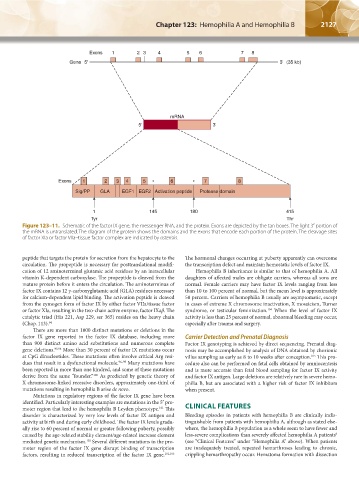
Figure 123–11. Schematic of the factor IX gene, the messenger RNA, and the protein. Exons are depicted by the tan boxes. The light 3′ portion of
the mRNA is untranslated. The diagram of the protein shows the domains and the exons that encode each portion of the protein. The cleavage sites
of factor XIa or factor VIIa–tissue factor complex are indicated by asterisks.
peptide that targets the protein for secretion from the hepatocyte to the The hormonal changes occurring at puberty apparently can overcome
circulation. The propeptide is necessary for posttranslational modifi- the transcription defect and maintain hemostatic levels of factor IX.
cation of 12 aminoterminal glutamic acid residues by an intracellular Hemophilia B inheritance is similar to that of hemophilia A. All
vitamin K-dependent carboxylase. The propeptide is cleaved from the daughters of affected males are obligate carriers, whereas all sons are
mature protein before it enters the circulation. The aminoterminus of normal. Female carriers may have factor IX levels ranging from less
factor IX contains 12 γ-carboxyglutamic acid (GLA) residues necessary than 10 to 100 percent of normal, but the mean level is approximately
for calcium-dependent lipid binding. The activation peptide is cleaved 50 percent. Carriers of hemophilia B usually are asymptomatic, except
from the zymogen form of factor IX by either factor VIIa/tissue factor in cases of extreme X chromosome inactivation, X mosaicism, Turner
or factor XIa, resulting in the two-chain active enzyme, factor IXaβ. The syndrome, or testicular feminization. When the level of factor IX
104
catalytic triad (His 221, Asp 229, ser 365) resides on the heavy chain activity is less than 25 percent of normal, abnormal bleeding may occur,
(Chap. 113). 94 especially after trauma and surgery.
There are more than 1000 distinct mutations or deletions in the
factor IX gene reported in the factor IX database, including more Carrier Detection and Prenatal Diagnosis
than 900 distinct amino acid substitutions and numerous complete Factor IX genotyping is achieved by direct sequencing. Prenatal diag-
gene deletions. 95,96 More than 30 percent of factor IX mutations occur nosis may be accomplished by analysis of DNA obtained by chorionic
at CpG dinucleotides. These mutations often involve critical Arg resi- villus sampling as early as 8 to 10 weeks after conception. This pro-
105
dues that result in a dysfunctional molecule. 96–99 Many mutations have cedure also can be performed on fetal cells obtained by amniocentesis
been reported in more than one kindred, and some of these mutations and is more accurate than fetal blood sampling for factor IX activity
derive from the same “founder.” As predicted by genetic theory of and factor IX antigen. Large deletions are relatively rare in severe hemo-
100
X chromosome- linked recessive disorders, approximately one-third of philia B, but are associated with a higher risk of factor IX inhibitors
mutations resulting in hemophilia B arise de novo. when present.
Mutations in regulatory regions of the factor IX gene have been
identified. Particularly interesting examples are mutations in the 5′ pro-
moter region that lead to the hemophilia B Leyden phenotype. This CLINICAL FEATURES
101
disorder is characterized by very low levels of factor IX antigen and Bleeding episodes in patients with hemophilia B are clinically indis-
activity at birth and during early childhood. The factor IX levels gradu- tinguishable from patients with hemophilia A, although as stated else-
ally rise to 60 percent of normal or greater following puberty, possibly where, the hemophilia B population as a whole seem to have fewer and
9
caused by the age-related stability element/age-related increase element less-severe complications than severely affected hemophilia A patients
mediated genetic mechanism. Several different mutations in the pro- (see “Clinical Features” under “Hemophilia A” above). When patients
102
moter region of the factor IX gene disrupt binding of transcription are inadequately treated, repeated hemarthroses leading to chronic,
factors, resulting in reduced transcription of the factor IX gene. 101,103 crippling hemarthropathy occur. Hematoma formation with dissection
Kaushansky_chapter 123_p2113-2132.indd 2127 9/21/15 4:36 PM