
Page 659 - Williams Hematology ( PDFDrive )
P. 659
634 Part VI: The Erythrocyte Chapter 43: Iron Deficiency and Overload 635
MCHC values in iron-deficiency anemia iron concentration has a diurnal rhythm; it decreases in late afternoon
and evening, reaching a nadir near 9 pm and increases to its maximum
36 between 7 and 10 am. This effect is rarely of sufficient magnitude to
136
influence diagnosis. Serum iron levels decrease at about the time of
menstrual bleeding 137,138 regardless of whether the bleeding is physio-
34 logic or induced by withdrawal of contraceptive hormonal preparations.
Importantly, the serum iron concentration is reduced in the presence
MCHC (g/dL) 32 of either acute or chronic inflammatory processes or malignancy
139
140
and following acute myocardial infarction.
141,142
The serum iron concen-
tration under these circumstances may be decreased sufficiently to sug-
30 gest iron deficiency. Conversely, during chemotherapy of malignancy,
the serum iron concentration may be quite elevated, as cytotoxic effects
of the drugs on erythroblasts inhibit erythropoiesis and related iron
28 uptake by erythroblasts. This effect is observed from the third to the
seventh day after inception of chemotherapy of a variety of tumors. 143
Normal or high concentrations of serum iron are commonly
0 2 4 6 8 10 12 observed even in patients with iron-deficiency anemia if such patients
Hemoglobin concentration (g/dL) receive iron medication before blood is drawn for these measurements.
Even multivitamin preparations, which commonly contain approxi-
MCV values in iron-deficiency anemia mately 18 mg of elemental iron per tablet, can result in this effect. Oral
100 iron medication should be withheld for 24 hours before blood samples
are obtained. Parenteral injection of iron dextran may result in a very
high serum iron concentration (e.g., 500 to 1000 mcg/dL), at least with
80
144
some methods, for several weeks. The elevation of serum iron lev-
els after infusion of sodium ferric gluconate or iron sucrose is of much
145
shorter duration.
60
MCV (fL) Iron-Binding Capacity and Transferrin Saturation
40
The iron-binding capacity is a measure of the amount of transferrin in
circulating blood. Normally, there is enough transferrin present in 100
20 mL serum to bind 4.4 to 8.0 μmol (250 to 450 mcg) of iron; because
the normal serum iron concentration is approximately 1.8 μmol/dL
(100 mcg/dL), transferrin may be found to be approximately one-third
0 saturated with iron. The unsaturated or latent iron-binding capacity
0 2 4 6 8 10 12 (UIBC) is easily measured with radioactive iron or by spectrophotometric
Hemoglobin concentration (g/dL)
techniques. The sum of the UIBC and the plasma iron represents total
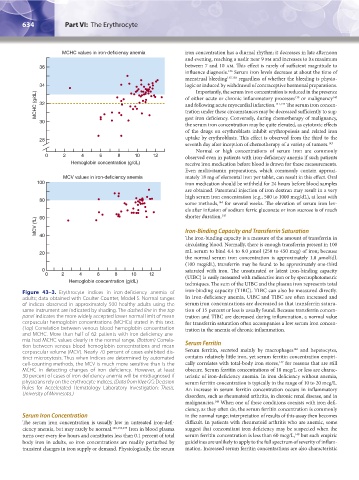
Figure 43–3. Erythrocyte indices in iron-deficiency anemia of iron-binding capacity (TIBC). TIBC can also be measured directly.
adults; data obtained with Coulter Counter, Model S. Normal ranges In iron-deficiency anemia, UIBC and TIBC are often increased and
of indices observed in approximately 500 healthy adults using the serum iron concentrations are decreased so that transferrin satura-
same instrument are indicated by shading. The dashed line in the top tion of 15 percent or less is usually found. Because transferrin concen-
panel indicates the more widely accepted lower normal limit of mean tration and TIBC are decreased during inflammation, a normal value
corpuscular hemoglobin concentrations (MCHCs) stated in this text. for transferrin saturation often accompanies a low serum iron concen-
(Top) Correlation between venous blood hemoglobin concentration tration in the anemia of chronic inflammation.
and MCHC. More than half of 62 patients with iron-deficiency ane-
mia had MCHC values clearly in the normal range. (Bottom) Correla-
tion between venous blood hemoglobin concentrations and mean Serum Ferritin
146
corpuscular volume (MCV). Nearly 70 percent of cases exhibited dis- Serum ferritin, secreted mainly by macrophages and hepatocytes,
tinct microcytosis. Thus when indices are determined by automated contains relatively little iron, yet serum ferritin concentration empiri-
147
cell-counting methods, the MCV is much more sensitive than is the cally correlates with total-body iron stores, for reasons that are still
MCHC in detecting changes of iron deficiency. However, at least obscure. Serum ferritin concentrations of 10 mcg/L or less are charac-
30 percent of cases of iron-deficiency anemia will be misdiagnosed if teristic of iron-deficiency anemia. In iron deficiency without anemia,
physicians rely on the erythrocyte indices. (Data from Klee GG: Decision serum ferritin concentration is typically in the range of 10 to 20 mcg/L.
Rules for Accelerated Hematology Laboratory Investigation: Thesis, An increase in serum ferritin concentration occurs in inflammatory
University of Minnesota.) disorders, such as rheumatoid arthritis, in chronic renal disease, and in
malignancies. When one of these conditions coexists with iron defi-
148
ciency, as they often do, the serum ferritin concentration is commonly
Serum Iron Concentration in the normal range; interpretation of results of this assay then becomes
The serum iron concentration is usually low in untreated iron-defi- difficult. In patients with rheumatoid arthritis who are anemic, some
ciency anemia, but may rarely be normal. 125,134,135 Iron in blood plasma suggest that concomitant iron deficiency may be suspected when the
turns over every few hours and constitutes less than 0.1 percent of total serum ferritin concentration is less than 60 mcg/L, but such empiric
149
body iron in adults, so iron concentrations are readily perturbed by guidelines are unlikely to apply to the full spectrum of severity of inflam-
transient changes in iron supply or demand. Physiologically, the serum mation. Increased serum ferritin concentrations are also characteristic
Kaushansky_chapter 43_p0627-0650.indd 634 9/17/15 6:27 PM