
Page 614 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 614
CHaPTEr 42 Urticaria, Angioedema, and Anaphylaxis 591
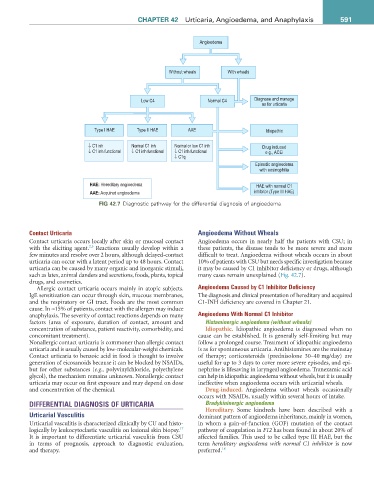
Angioedema
Without wheals With wheals
Low C4 Normal C4 Diagnose and manage
as for urticaria
Type I HAE Type II HAE AAE Idiopathic
↓ C1 inh Normal C1 inh Normal or low C1 inh Drug induced
↓ C1 inh functional ↓ C1 inh functional ↓ C1 inh functional e.g., ACEi
↓ C1q
Episodic angioedema
with eosinophilia
HAE: Hereditary angioedema HAE with normal C1
AAE: Acquired angioedema inhibitor (Type III HAE)
fiG 42.7 Diagnostic pathway for the differential diagnosis of angioedema.
Contact Urticaria Angioedema Without Wheals
Contact urticaria occurs locally after skin or mucosal contact Angioedema occurs in nearly half the patients with CSU; in
2,3
with the eliciting agent. Reactions usually develop within a these patients, the disease tends to be more severe and more
few minutes and resolve over 2 hours, although delayed-contact difficult to treat. Angioedema without wheals occurs in about
urticaria can occur with a latent period up to 48 hours. Contact 10% of patients with CSU but needs specific investigation because
urticaria can be caused by many organic and inorganic stimuli, it may be caused by C1 inhibitor deficiency or drugs, although
such as latex, animal danders and secretions, foods, plants, topical many cases remain unexplained (Fig. 42.7).
drugs, and cosmetics.
Allergic contact urticaria occurs mainly in atopic subjects. Angioedema Caused by C1 Inhibitor Deficiency
IgE sensitization can occur through skin, mucous membranes, The diagnosis and clinical presentation of hereditary and acquired
and the respiratory or GI tract. Foods are the most common C1-INH deficiency are covered in Chapter 21.
cause. In ≈15% of patients, contact with the allergen may induce
anaphylaxis. The severity of contact reactions depends on many Angioedema With Normal C1 Inhibitor
factors (area of exposure, duration of contact, amount and Histaminergic angioedema (without wheals)
concentration of substance, patient reactivity, comorbidity, and Idiopathic. Idiopathic angioedema is diagnosed when no
concomitant treatment). cause can be established. It is generally self-limiting but may
Nonallergic contact urticaria is commoner than allergic contact follow a prolonged course. Treatment of idiopathic angioedema
urticaria and is usually caused by low-molecular-weight chemicals. is as for spontaneous urticaria. Antihistamines are the mainstay
Contact urticaria to benzoic acid in food is thought to involve of therapy; corticosteroids (prednisolone 30–40 mg/day) are
generation of eicosanoids because it can be blocked by NSAIDs, useful for up to 3 days to cover more severe episodes, and epi-
but for other substances (e.g., polyvinylchloride, polyethylene nephrine is lifesaving in laryngeal angioedema. Tranexamic acid
glycol), the mechanism remains unknown. Nonallergic contact can help in idiopathic angioedema without wheals, but it is usually
urticaria may occur on first exposure and may depend on dose ineffective when angioedema occurs with urticarial wheals.
and concentration of the chemical. Drug-induced. Angioedema without wheals occasionally
occurs with NSAIDs, usually within several hours of intake.
DIFFERENTIAL DIAGNOSIS OF URTICARIA Bradykininergic angioedema
Hereditary. Some kindreds have been described with a
Urticarial Vasculitis dominant pattern of angioedema inheritance, mainly in women,
Urticarial vasculitis is characterized clinically by CU and histo- in whom a gain-of-function (GOF) mutation of the contact
17
logically by leukocytoclastic vasculitis on lesional skin biopsy. pathway of coagulation in F12 has been found in about 20% of
It is important to differentiate urticarial vasculitis from CSU affected families. This used to be called type III HAE, but the
in terms of prognosis, approach to diagnostic evaluation, term hereditary angioedema with normal C1 inhibitor is now
and therapy. preferred. 18