
Page 766 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 766
738 ParT Six Systemic Immune Diseases
Parasympathetic nerve Chronic xerostomia necessitates the use of fluids throughout
the day and night. It is not uncommon for patients with SS to
wake up at night to drink fluids to relieve dryness and also to
DAG require the use of fluids to be able to speak, chew, and swallow.
PIP2
M3R A burning sensation along with taste alterations and decreased
ACh
tolerance to spicy foods is described by a significant percentage
Na + PLC + Interstitium of patients.
Head and neck examination often reveals dry and chapped
K + lips, angular cheilitis, and swollen major salivary glands (Fig.
54.3), which may be recurrent or chronic. Intraoral findings
G g /G 11 include decreased salivary pooling under the tongue and a
IP 3 depapillated tongue surface often associated with erythematous
STIM1 candidiasis (Fig. 54.4). Vasculitis can also manifest in the oral
IP3R cavity and lead to tissue breakdown. Teeth often exhibit an
Ca 2+ increased rate of caries with characteristic decay affecting the
Ca 2+ roots and cusp tips (Fig. 54.5).
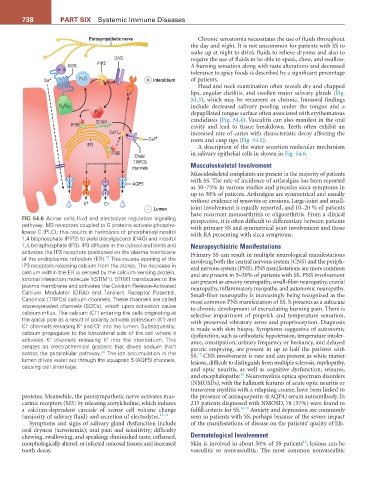
ER A description of the water secretion molecular mechanism
IP3R in salivary epithelial cells in shown in Fig. 54.6.
Orais/
TRPCS
channels Musculoskeletal Involvement
Musculoskeletal complaints are present in the majority of patients
with SS. The rate of incidence of arthralgias has been reported
AQP5
as 50–75% in various studies and precedes sicca symptoms in
up to 30% of patients. Arthralgias are symmetrical and usually
K + Cl – without evidence of synovitis or erosions. Large-joint and small-
− Lumen joint involvement is equally reported, and 10–20 % of patients
have recurrent monoarthritis or oligoarthritis. From a clinical
FiG 54.6 Acinar cells fluid and electrolyte regulation signaling perspective, it is often difficult to differentiate between patients
pathway. M3 receptors coupled to G proteins activate phospho- with primary SS and symmetrical joint involvement and those
lipase C (PLC); this results in hydrolysis of phosphatidylinositol with RA presenting with sicca symptoms.
1,4 bisphosphate (PIP2) to yield diacylglycerol (DAG) and inositol
1,4,5-trisphosphate (IP3). IP3 diffuses in the cytosol and binds and Neuropsychiatric Manifestations
activates the IP3 receptors positioned on the plasma membrane Primary SS can result in multiple neurological manifestations
of the endoplasmic reticulum (ER). This causes opening of the involving both the central nervous system (CNS) and the periph-
19
IP3 receptors releasing calcium from the stores. The decrease in eral nervous system (PNS). PNS manifestations are more common
calcium within the ER is sensed by the calcium sensing protein, and are present in 5–20% of patients with SS. PNS involvement
stromal interaction molecule 1(STIM1). STIM1 translocates to the can present as sensory neuropathy, small-fiber neuropathy, cranial
plasma membrane and activates the Calcium Release-Activated neuropathy, inflammatory myopathy, and autonomic neuropathy.
Calcium Modulator (ORAI) and Tansient Receptor Potential, Small-fiber neuropathy is increasingly being recognized as the
Canonical (TRPCs) calcium channels. These channels are called most common PNS manifestation of SS. It presents as a subacute
store-operated channels (SOCs), which upon activation cause to chronic development of excruciating burning pain. There is
−
calcium influx. The calcium (Cl ) entering the cells originating at selective impairment of pinprick and temperature sensation,
+
the apical pole as a result of polarity activate potassium (K ) and with preserved vibratory sense and proprioception. Diagnosis
−
+
−
Cl channels releasing K and Cl into the lumen. Subsequently, is made with skin biopsy. Symptoms suggestive of autonomic
calcium propagates to the basolateral side of the cell where it dysfunction, such as orthostatic hypotension, temperature intoler-
+
+
activates K channels releasing K into the interstitium. This ance, constipation, urinary frequency or hesitancy, and delayed
+
creates an electrochemical gradient that drives sodium (Na ) gastric emptying, are present in up to half the patients with
20
across the paracellular pathway. The ion accumulation in the SS. CNS involvement is rare and can present as white matter
15
lumen drives water out through the aquaporin 5 (AQP5) channels, lesions, difficult to distinguish from multiple sclerosis, myelopathy,
causing cell shrinkage.
and optic neuritis, as well as cognitive dysfunction, seizures,
15
and encephalopathy. Neuromyelitis optica spectrum disorders
(NMOSDs), with the hallmark features of acute optic neuritis or
transverse myelitis with a relapsing course, have been linked to
proteins. Meanwhile, the parasympathetic nerve activates mus- the presence of antiaquaporin-4(AQP4) serum autoantibody. In
carinic receptors (M3) by releasing acetylcholine, which induces 213 patients diagnosed with NMOSD, 78 (37%) were found to
a calcium-dependent cascade of acinar cell volume change fulfill criteria for SS. 16-18 Anxiety and depression are commonly
(majority of salivary fluid) and secretion of electrolytes. 12-14 seen in patients with SS, perhaps because of the severe impact
Symptoms and signs of salivary gland dysfunction include of the manifestations of disease on the patients’ quality of life.
oral dryness (xerostomia); oral pain and sensitivity; difficulty
chewing, swallowing, and speaking; diminished taste; inflamed, Dermatological Involvement
19
morphologically altered, or infected mucosal tissues; and increased Skin is involved in about 50% of SS patients ; lesions can be
tooth decay. vasculitic or nonvasculitic. The most common nonvasculitic