
Page 1151 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1151
790 PART 6: Neurologic Disorders
increases by extruding blood out of the intracranial space. First, the less
200 C
resistant cerebral venous system reduces its blood volume, and then the
180 circulation within the arterial tree is reduced. Lastly, brain parenchyma
will follow by shifting along the ICP gradient within the cranial vault
Intracranial pressure 160 P V and away from the space-occupying lesion. This is described as brain
140
herniation. Herniation syndromes can be distinguished clinically and
120
radiographically depending on which vector the ICP gradient contin-
ues to evolve, that is, from one to the opposite hemisphere or along the
100
80
The important concepts of ICP-volume relationships and intra-
60 craniocaudal cerebrospinal axis.
A B cranial compliance can be applied to the radiographic estimation of
40 V the likelihood of intracranial hypertension from a space-occupying
20 P intracranial process to determine the indication for invasive pres-
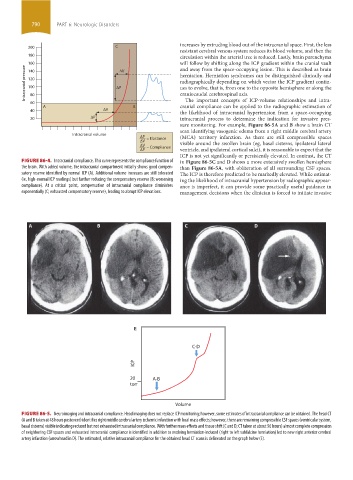
sure monitoring. For example, Figure 86-5A and B show a brain CT
scan identifying vasogenic edema from a right middle cerebral artery
Intracranial volume
P = Elastance (MCA) territory infarction. As there are still compressible spaces
V visible around the swollen brain (eg, basal cisterns, ipsilateral lateral
V = Compliance
P ventricle, and ipsilateral cortical sulci), it is reasonable to expect that the
ICP is not yet significantly or persistently elevated. In contrast, the CT
FIGURE 86-4. Intracranial compliance. This curve represents the compliance function of in Figure 86-5C and D shows a more extensively swollen hemisphere
the brain. With added volume, the intracranial compartment initially shows good compen- than Figure 86-5A, with obliteration of all surrounding CSF spaces.
satory reserve identified by normal ICP (A). Additional volume increases are still tolerated The ICP is therefore predicted to be markedly elevated. While estimat-
(ie, high-normal ICP readings) but further reducing the compensatory reserve (B; worsening ing the likelihood of intracranial hypertension by radiographic appear-
compliance). At a critical point, compensation of intracranial compliance diminishes ance is imperfect, it can provide some practically useful guidance in
exponentially (C; exhausted compensatory reserve), leading to abrupt ICP elevations. management decisions when the clinician is forced to initiate invasive
A B C D
E
C-D
ICP
20 A-B
torr
Volume
FIGURE 86-5. Neuroimaging and intracranial compliance. Head imaging does not replace ICP monitoring; however, some estimates of intracranial compliance can be obtained. The head CT
(A and B taken at 48 hours postevent) identifies right middle cerebral artery ischemic infarction with local mass effects; however, there are remaining compressible CSF spaces (ventricular system,
basal cisterns) visible indicating reduced but not exhausted intracranial compliance. With further mass effects and tissue shift (C and D; CT taken at about 96 hours) almost complete compression
of neighboring CSF spaces and exhausted intracranial compliance is identified in addition to evolving herniation-induced (right to left subfalcine herniation) led to new right anterior cerebral
artery infarction (arrowhead in D). The estimated, relative intracranial compliance for the obtained head CT scans is delineated on the graph below (E).
section06.indd 790 1/23/2015 12:55:48 PM