
Page 527 - Clinical Hematology_ Theory _ Procedures ( PDFDrive )
P. 527
CHAPTER 26 ■ Disorders of Primary Hemostasis and Thrombosis Vasculature and Platelets 511
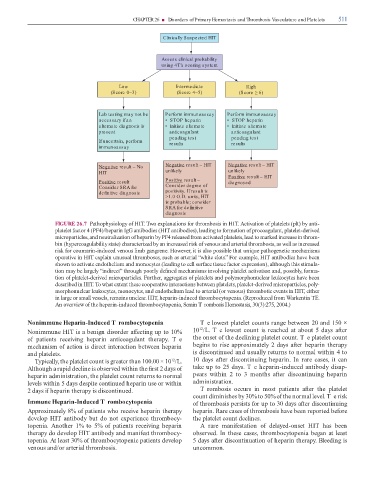
Clinically Suspected HIT
Assess clinical probability
using 4T’s scoring system
Low Intermediate High
(Score 0–3) (Score 4–5) (Score ≥ 6)
Lab testing may not be Perform immunoassay Perform immunoassay
necessary if an • STOP heparin • STOP heparin
alternate diagnosis is • Initiate alternate • Initiate alternate
present anticoagulant anticoagulant
pending test pending test
If uncertain, perform results results
immunoassay
Negative result – No Negative result – HIT Negative result – HIT
HIT unlikely unlikely
Positive result – HIT
Positive result – Positive result – diagnosed
Consider SRA for Consider degree of
definitive diagnosis positivity. If result is
>1.0 O.D. units, HIT
is probable; consider
SRA for definitive
diagnosis
FIGURE 26.7 Patho hysio ogy o HI . wo ex anations or thro bosis in HI . Activation o ate ets ( t) by anti-
ate et actor 4 (PF4)/he arin IgG antibo ies (HI antibo ies), ea ing to or ation o rocoagu ant, ate et- erive
icro artic es, an neutra ization o he arin by PF4 re ease ro activate ate ets, ea to arke increase in thro -
bin (hy ercoagu abi ity state) characterize by an increase risk o venous an arteria thro bosis, as we as increase
risk or cou arin-in uce venous i b gangrene. However, it is a so ossib e that unique athogenetic echanis s
o erative in HI ex ain unusua thro boses, such as arteria “white c ots.” For exa e, HI antibo ies have been
shown to activate en othe iu an onocytes ( ea ing to ce sur ace tissue actor ex ression), a though this sti u a-
tion ay be arge y “in irect” through oor y e ne echanis s invo ving ate et activation an , ossib y, or a-
tion o ate et- erive icro artic es. Further, aggregates o ate ets an o y or honuc ear eukocytes have been
escribe in HI . o what extent these coo erative interactions between ate ets, ate et- erive icro artic es, o y-
or honuc ear eukocytes, onocytes, an en othe iu ea to arteria (or venous) thro botic events in HI , either
in arge or s a vesse s, re ains unc ear. HI , he arin-in uce thro bocyto enia. (Re ro uce ro Warkentin E.
An overview o the he arin-in uce thro bocyto enia, Semin T rombosis Hemostasis, 30(3):275, 2004.)
Nonimmune Heparin-Induced T rombocytopenia Te owest ate et counts range between 20 an 150 ×
12
Noni une HI is a benign isor er a ecting u to 10% 10 /L. T e owest count is reache at about 5 ays a er
o atients receiving he arin anticoagu ant thera y. T e the onset o the ec ining ate et count. T e ate et count
echanis o action is irect interaction between he arin begins to rise a roxi ate y 2 ays a er he arin thera y
an ate ets. is iscontinue an usua y returns to nor a within 4 to
y ica y, the ate et count is greater than 100.00 × 10 /L. 10 ays a er iscontinuing he arin. In rare cases, it can
12
A though a ra i ec ine is observe within the rst 2 ays o take u to 25 ays. T e he arin-in uce antibo y isa -
he arin a inistration, the ate et count returns to nor a ears within 2 to 3 onths a er iscontinuing he arin
eve s within 5 ays es ite continue he arin use or within a inistration.
2 ays i he arin thera y is iscontinue . T ro bosis occurs in ost atients a er the ate et
count i inishes by 30% to 50% o the nor a eve . T e risk
Immune Heparin-Induced T rombocytopenia o thro bosis ersists or u to 30 ays a er iscontinuing
A roxi ate y 8% o atients who receive he arin thera y he arin. Rare cases o thro bosis have been re orte be ore
eve o HI antibo y but o not ex erience thro bocy- the ate et count ec ines.
to enia. Another 1% to 5% o atients receiving he arin A rare ani estation o e aye -onset HI has been
thera y o eve o HI antibo y an ani est thro bocy- observe . In these cases, thro bocyto enia began at east
to enia. At east 30% o thro bocyto enic atients eve o 5 ays a er iscontinuation o he arin thera y. B ee ing is
venous an /or arteria thro bosis. unco on.