
Page 143 - Textbook of Pathology, 6th Edition
P. 143
pleuritis usually covers the area of infarct. Cut surface is 127
dark purple and may show the blocked vessel near the
apex of the infarcted area. Old organised and healed
pulmonary infarcts appear as retracted fibrous scars.
Microscopically, the characteristic histologic feature is
coagulative necrosis of the alveolar walls. Initially, there CHAPTER 5
is infiltration by neutrophils and intense alveolar capillary
congestion, but later their place is taken by haemosiderin,
phagocytes and granulation tissue (Fig. 5.28).
INFARCT KIDNEY. Renal infarction is common, found in
up to 5% of autopsies. Majority of them are caused by
thromboemboli, most commonly originating from the heart
such as in mural thrombi in the left atrium, myocardial
infarction, vegetative endocarditis and from aortic aneurysm.
Less commonly, renal infarcts may occur due to advanced
renal artery atherosclerosis, arteritis and sickle cell anaemia.
Grossly, renal infarcts are often multiple and may be
bilateral. Characteristically, they are pale or anaemic and
wedge-shaped with base resting under the capsule and
apex pointing towards the medulla. Generally, a narrow
rim of preserved renal tissue under the capsule is spared
because it draws its blood supply from the capsular Derangements of Homeostasis and Haemodynamics
vessels. Cut surface of renal infarct in the first 2 to 3 days
is red and congested but by 4th day the centre becomes
pale yellow. At the end of one week, the infarct is typically
anaemic and depressed below the surface of the kidney
Figure 5.26 Common locations of systemic infarcts following arterial (Fig. 5.29).
embolism.
Microscopically, the affected area shows characteristic
coagulative necrosis of renal parenchyma i.e. there are
who have inadequate circulation such as in chronic lung ghosts of renal tubules and glomeruli without intact nuclei
diseases and congestive heart failure.
and cytoplasmic content. The margin of the infarct shows
inflammatory reaction—initially acute but later
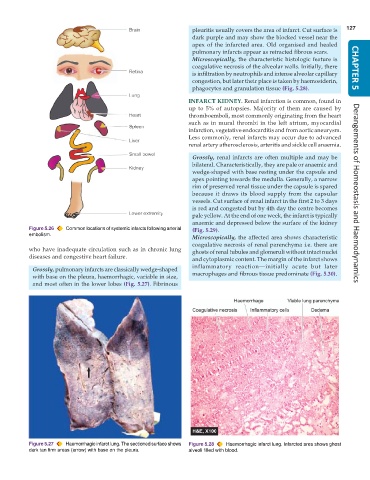
Grossly, pulmonary infarcts are classically wedge-shaped
with base on the pleura, haemorrhagic, variable in size, macrophages and fibrous tissue predominate (Fig. 5.30).
and most often in the lower lobes (Fig. 5.27). Fibrinous
Figure 5.27 Haemorrhagic infarct lung. The sectioned surface shows Figure 5.28 Haemorrhagic infarct lung. Infarcted area shows ghost
dark tan firm areas (arrow) with base on the pleura. alveoli filled with blood.