
Page 18 - 2021 Team Member Benefit Guide - English
P. 18
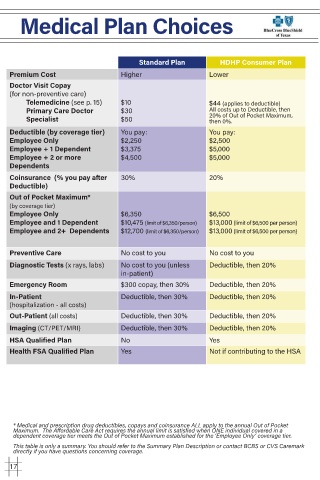
Medical Plan Choices
Standard Plan HDHP Consumer Plan
Premium Cost Higher Lower
Doctor Visit Copay
(for non-preventive care)
Telemedicine (see p. 15) $10 $44 (applies to deductible)
Primary Care Doctor $30 All costs up to Deductible, then
Specialist $50 20% of Out of Pocket Maximum,
then 0%.
Deductible (by coverage tier) You pay: You pay:
Employee Only $2,250 $2,500
Employee + 1 Dependent $3,375 $5,000
Employee + 2 or more $4,500 $5,000
Dependents
Coinsurance (% you pay after 30% 20%
Deductible)
Out of Pocket Maximum*
(by coverage tier)
Employee Only $6,350 $6,500
Employee and 1 Dependent $10,475 (limit of $6,350/person) $13,000 (limit of $6,500 per person)
Employee and 2+ Dependents $12,700 (limit of $6,350/person) $13,000 (limit of $6,500 per person)
Preventive Care No cost to you No cost to you
Diagnostic Tests (x rays, labs) No cost to you (unless Deductible, then 20%
in-patient)
Emergency Room $300 copay, then 30% Deductible, then 20%
In-Patient Deductible, then 30% Deductible, then 20%
(hospitalization - all costs)
Out-Patient (all costs) Deductible, then 30% Deductible, then 20%
Imaging (CT/PET/MRI) Deductible, then 30% Deductible, then 20%
HSA Qualified Plan No Yes
Health FSA Qualified Plan Yes Not if contributing to the HSA
* Medical and prescription drug deductibles, copays and coinsurance ALL apply to the annual Out of Pocket
Maximum. The Affordable Care Act requires the annual limit is satisfied when ONE individual covered in a
dependent coverage tier meets the Out of Pocket Maximum established for the ‘Employee Only’ coverage tier.
This table is only a summary. You should refer to the Summary Plan Description or contact BCBS or CVS Caremark
directly if you have questions concerning coverage.
17