
Page 244 - fbkCardioDiabetes_2017
P. 244
220 Cardio Diabetes Medicine 2017
Pre Diabetes as Risk Factor for Coronary Artery
Disease & Peripheral Vascular Disease.
Dr. Arulprakash,
MD., MRCP(UK)., FRCP(Lon).,
Indra diabetes Centre, Tuticorin
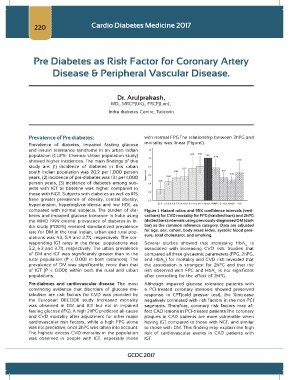
Prevalence of Pre diabetes: with normal FPG.The relationship between 2hPG and
Prevalence of diabetes, impaired fasting glucose mortality was linear (Figure1).
and insulin resistance syndrome in an urban Indian
population (CUPS- Chennai Urban population study)
showed higher incidences. The main findings of this
study are: (1) incidence of diabetes in this urban
south Indian population was 20.2 per 1,000 person
years, (2) incidence of pre-diabetes was 13.1 per 1,000
person years, (3) incidence of diabetes among sub-
jects with IGT at baseline was higher compared to
those with NGT. Subjects with diabetes as well as IRS
have greater prevalence of obesity, central obesity,
hypertension, hypertriglyceridemia and low HDL as
compared with normal subjects. The burden of dia- Figure 1. Hazard ratios and 95% confidence intervals (verti-
betes and impaired glucose tolerance in India using cal bars) for CVD mortality for FPG (hatched bars) and 2hPG
the WHO 1999 criteria: prevalence of diabetes in In- (dotted bars) intervals using previously diagnosed DM (dark
dia study (PODIS) revealed standardized prevalence bar) as the common reference category. Data are adjusted
rate for DM in the total Indian, urban and rural pop- for age, sex, cohort, body mass index, systolic blood pres-
ulations was 4.3, 5.9 and 2.7%, respectively. The cor- sure, total cholesterol, and smoking.
responding IGT rates in the three populations was Several studies showed that increasing HbA is
1c
5.2, 6.3 and 3.7%, respectively. The urban prevalence associated with increasing CVD risk. Studies that
of DM and IGT was significantly greater than in the compared all three glycaemic parameters (FPG, 2hPG,
rural population (P < 0.001 in both instances). The and HbA ) for mortality and CVD risk revealed that
1c
prevalence of DM was significantly, more than that the association is strongest for 2hPG and that the
of IGT (P < 0.001) within both the rural and urban risk observed with FPG and HbA is not significant
1c
populations. after controlling for the effect of 2hPG.
Pre-diabetes and cardiovascular disease: The most Although impaired glucose tolerance patients with
convincing evidence that disorders of glucose me- a PCI-treated coronary stenosis showed preserved
tabolism are risk factors for CVD was provided by response to CPT(cold pressor test), the %increase
the European DECODE study. Increased mortality negatively correlated with risk factors in the non-PCI
was observed in DM and IGT but not in impaired segments. Therefore, coronary risk factors may af-
fasting glucose (IFG). A high 2hPG predicted all-cause fect CAD lesions in PCI-treated patients.The coronary
and CVD mortality after adjustment for other major plaques in CAD patients are more vulnerable when
cardiovascular risk factors, while a high FPG alone having IGT compared to those with NGT, and similar
was not predictive, once 2hPG was taken into account. to those with DM. This finding may explain the high
The highest excess CVD mortality in the population risk of cardiovascular events in CAD patients with
was observed in people with IGT, especially those IGT.
GCDC 2017