
Page 1160 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1160
Doll’s eye maneuver:
Upper pons
pontine hemorrhage,
Impaired, may be dysconjugate
focal pathology within the
Ice water calorics:
pons caused by shearing
Impaired, may be dysconjugate
Apneusis
injury, demyelination,
Pinpoint poorly reactive pupils
increased ICP leading to
pontine involvement
Lower pons
Lower pontine injury
Doll’s eye maneuver:
No response
Ice water calorics:
No response Cluster breathing Examples: secondary to
Eupneic, although often
more shallow and rapid
than normal
Upper medulla Doll’s eye maneuver: If medullary involvement
No response alone, this is associated
with dysarthria,
Ice water calorics: ?? dysphagia,poor cough,
No response
Flaccid
and gag reflex
Midposition and fixed CHAPTER 86: Intracranial Pressure: Monitoring and Management 799
Slow, irregular rate and
amplitude If due to elevated ICP
and with medullary
(Ataxic breathing)
involvement, there will be
TABLE 86-5 Neurologic Examination in Comatose Patients (Continued) impaired consciousness
Cervical spine Doll’s eye maneuver: Disruption of sympathetic
(Avoid with cervical lesion) nervous system caused
by spinal cord lesion
Ice water calorics: above the first thoracic
Present
Horner pupil vertebra
(composed of ptosis,
miosis, and anhidrosis) Nonspecific
Severe Opisthotonus posturing
brainstem seen usually in infants,
lesion/ secondary to disinhibited
extra pyramidal Nonspecific Nonspecific extrapyramidal activity
lesion caused by axial spinal
Opisthotonus posturing muscles spasm
ICP, intracranial pressure; PCA, posterior cerebral artery; Pcomm, posterior communicating artery.
Summary of important neurological findings seen in comatose patients. ICP, intracranial pressure; PCA, posterior cerebral artery; Pcomm, posterior communicating artery
respiratory irregularity commonly presenting as irregular tachypnea. (eg, abnormalities of the cranial nerves, motor, and peripheral reflex
Only approximately one-third of patients demonstrate all signs of the examinations). Papilledema, defined as edema of the optic nerve that
triad. Careful observation of the breathing pattern can help define extends anteriorly and laterally into the vitreous humor, is an important
whether ICP is the etiology of the abnormality and can localize the and reliable manifestation of raised ICP. It may be asymptomatic in its
level of injury (Table 86-5). This “autonomic survey” and search for any early stages, but when sustained inevitably progresses to enlargement
spontaneous patient movements is often followed by the assessment of a of the blind spot, blurring of vision, visual obscurations, and ultimately
patient’s level of arousal. There are several scales and terms to classify the total loss of vision. It usually develops over days to weeks, and is there-
level of consciousness (Table 86-6). The Glasgow Coma Scale provides a fore not a manifestation of acute intracranial hypertension in patients
rapid and universal language when describing the degree of brain injury with head injury. In a study of patients with head trauma, 54% of
and this classification system should be a component of any intensive patients had increased ICP, but only 3.5% had papilledema on fundo-
care physician’s diagnostic tool set. scopic examination. Fundoscopic examination reveals loss of venous
31
Following the assessment of the level of alertness and cognitive pulsation, venous engorgement, optic disc hemorrhage, increased
function other findings indicative for elevated ICP should be sought diameter of the optic nerve head, and blurring of its margins at the optic
A C TABLE 86-6 level of Consciousness
level Other Names Description
Conscious “Normal” Spontaneously awake and alert, promptly
stating name, location, date, and time
(oriented to three spheres)
Confused Disoriented; impaired Slow in response with memory time loss,
thought processing and confused, disoriented, difficulty following
responsiveness; “clouding instruction, delayed responses
of consciousness”
B D Delirious Disoriented; marked loss Also mixture of episodic agitation,
of attention, restless, somnolence, and obtundation with restlessness
illusions, hallucinations, or agitation, marked deficits in attention and
delusions concentration
Somnolent Drowsiness, state of Dozes after stimuli; incoherent mumbling or
near-sleep disorganized movements observed but still able
to follow simple commands upon stimulation
Obtunded Mentally dulled, decreased Decreased interest in surroundings, slowed
alertness and psychomotor responses, only brief arousal, unable to
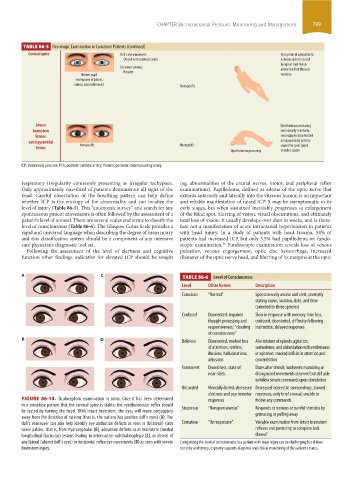
FIGURE 86-14. Oculocephalic examination in coma. Once it has been determined responses follow any commands
in a comatose patient that the cervical spine is stable, the vestibuloocular reflex should Stuporous “Nonspontaneous” Responds to noxious or painful stimulus by
be tested by turning the head. With intact brainstem, the eyes will move conjugately
away from the direction of turning (that is, the patient has positive doll’s eyes) (A). The grimacing or pulling away
doll’s maneuver can also help identify eye abduction deficits as seen in (bilateral) sixth Comatose “Unresponsive” Variable examination from intact brainstem
nerve palsies, that is, from hydrocephalus (B), adduction deficits as in brainstem (medial reflexes and posturing to complete lack
longitudinal fasciculus) lesions leading to internuclear ophthalmoplegia (C), or absent of thereof
any lateral (absent doll’s eyes) or horizontal reflex eye movements (D) as seen with severe Categorizing the level of consciousness in a patient with brain injury can be challenging but if done
brainstem injury. correctly and timely, it greatly supports diagnosis and clinical monitoring of the patient’s status.
section06.indd 799 1/23/2015 12:56:01 PM