
Page 82 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 82
50 PART 1: An Overview of the Approach to and Organization of Critical Care
Medical informatics
Public health informatics
Epidemiology Personal health records
Biostatistics
Computer science Bioinformatics Security/Policy Clinical informatics Interoperability
Clinical informatics
Imaging
Clinical data warehousing
Enrollment to Carrying management Standards
clinical trials clinical trials
Biomedical Medical
Engineering Physics
Cognitive science
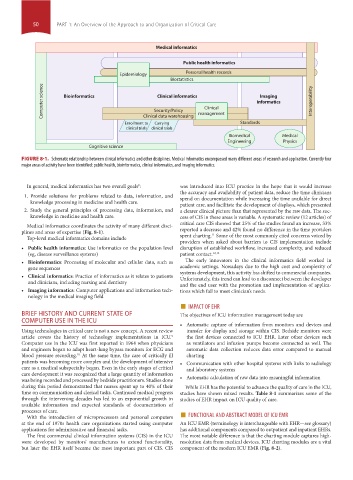
FIGURE 8-1. Schematic relationship between clinical informatics and other disciplines. Medical informatics encompassed many different areas of research and application. Currently four
major areas of activity have been identified: public health, bioinformatics, clinical informatics, and imaging informatics.
In general, medical informatics has two overall goals : 8 was introduced into ICU practice in the hope that it would increase
the accuracy and availability of patient data, reduce the time clinicians
1. Provide solutions for problems related to data, information, and spend on documentation while increasing the time available for direct
knowledge processing in medicine and health care. patient care, and facilitate the development of displays, which presented
2. Study the general principles of processing data, information, and a clearer clinical picture than that represented by the raw data. The suc-
knowledge in medicine and health care. cess of CIS in these areas is variable. A systematic review (12 articles) of
critical care CIS showed that 25% of the studies found an increase, 33%
Medical informatics coordinates the activity of many different disci-
plines and areas of expertise (Fig. 8-1). reported a decrease and 42% found no difference in the time providers
11
Top-level medical informatics domains include spent charting. Some of the most commonly cited concerns voiced by
providers when asked about barriers to CIS implementation include
• Public health informatics: Use informatics on the population level disruption of established workflow, increased complexity, and reduced
(eg, disease surveillance systems) patient contact. 12,13
• Bioinformatics: Processing of molecular and cellular data, such as The early innovators in the clinical informatics field worked in
gene sequences academic settings. Nowadays due to the high cost and complexity of
• Clinical informatics: Practice of informatics as it relates to patients systems development, this activity has shifted to commercial companies.
Unfortunately, this trend can lead to a disconnect between the developer
and clinicians, including nursing and dentistry and the end user with the promotion and implementation of applica-
• Imaging informatics: Computer applications and information tech- tions which fail to meet clinician’s needs.
nology in the medical imaging field
■ IMPACT OF EHR
BRIEF HISTORY AND CURRENT STATE OF The objectives of ICU information management today are
COMPUTER USE IN THE ICU
• Automatic capture of information from monitors and devices and
Using technologies in critical care is not a new concept. A recent review transfer for display and storage within CIS. Bedside monitors were
article covers the history of technology implementations in ICU. the first devices connected to ICU EHR. Later other devices such
9
Computer use in the ICU was first reported in 1964 when physicians as ventilators and infusion pumps become connected as well. The
and engineers began to adapt heart-lung bypass monitors for ECG and automatic data collection reduces data error compared to manual
blood pressure recording. At the same time, the care of critically ill charting
10
patients was becoming more complex and the development of intensive • Communication with other hospital systems with links to radiology
care as a medical subspecialty began. Even in the early stages of critical and laboratory systems
care development it was recognized that a large quantity of information
was being recorded and processed by bedside practitioners. Studies done • Automatic calculation of raw data into meaningful information
during this period demonstrated that nurses spent up to 40% of their While EHR has the potential to advance the quality of care in the ICU,
time on communication and clerical tasks. Continued medical progress studies have shown mixed results. Table 8-1 summarizes some of the
through the intervening decades has led to an exponential growth in studies of EHR impact on ICU quality of care.
available information and expected standards of documentation of
With the introduction of microprocessors and personal computers ■
processes of care. FUNCTIONAL AND ABSTRACT MODEL OF ICU EMR
at the end of 1970s health care organizations started using computer An ICU EMR (terminology is interchangeable with EHR—see glossary)
applications for administrative and financial tasks. has additional components compared to outpatient and inpatient EHRs.
The first commercial clinical information systems (CIS) in the ICU The most notable difference is that the charting module captures high-
were developed by monitors’ manufactures to extend functionality, resolution data from medical devices. ICU charting modules are a vital
but later the EHR itself became the most important part of CIS. CIS component of the modern ICU EMR (Fig. 8-2).
Section01.indd 50 1/22/2015 9:36:59 AM