
Page 898 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 898
CHAPTER 69: Human Immunodeficiency Virus (HIV) and AIDS in the Intensive Care Unit 629
unexplained extensive herpes zoster, or persistent generalized lymph-
adenopathy combined with a history (or clinical evidence) of high-risk
activities must trigger consideration of HIV infection in the differen-
tial diagnosis. Furthermore, laboratory abnormalities found commonly
among HIV-infected individuals can provide the clues to consider HIV
infection. Common laboratory abnormalities in HIV-infected patients
include lymphopenia, anemia, thrombocytopenia, and hypergamma-
globulinemia. It must be emphasized, however, that HIV infection should
not be diagnosed unless HIV has been confirmed using specific serologic
tests, most commonly, enzyme-linked immunosorbent assay (ELISA) and
Western blot. We reemphasize that universal precautions must be followed
https://kat.cr/user/tahir99/
by all clinical staff caring for ICU (and indeed all hospitalized) patients.
APPROACH TO THE HIV-INFECTED PATIENT IN THE ICU
■ RESPIRATORY DISEASE COMPLICATING HIV INFECTION
Pulmonary and radiologic manifestations of HIV infection are diverse and
include both infectious and noninfectious conditions (see Table 69-3).
62
Bacterial pneumonias remain most common causes of pulmonary infec-
tion and cause considerable morbidity and mortality worldwide. 63,64
The most common etiology of bacterial pneumonia in HIV-infected
individuals is Streptococcus pneumoniae, followed by Haemophilus
influenzae. 63,65,66 Other bacterial agents identified in the setting of
HIV-related bacterial pneumonia include Pseudomonas aeruginosa,
Staphylococcus aureus, and less commonly Legionella pneumophila. 65,67-69
The rates of hospitalization for pneumonia have decreased. Population-
based national data from Denmark demonstrated that hospitalization
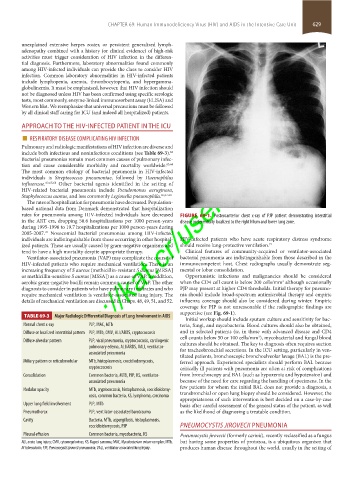
rates for pneumonia among HIV-infected individuals have decreased FIGURE 69-1. Posteroanterior chest x-ray of PJP patient demonstrating interstitial
in the ART era, dropping 50.6 hospitalizations per 1000 person-years disease preferentially localized to the right hilum and lower lung zone.
during 1995-1996 to 19.7 hospitalizations per 1000 person-years during
2005-2007. Nosocomial bacterial pneumonias among HIV-infected
70
individuals are indistinguishable from those occurring in other hospital- HIV-infected patients who have acute respiratory distress syndrome
ized patients. These are usually caused by gram-negative organisms and should receive lung-protective ventilation. 71
tend to have a high mortality despite appropriate therapy. Clinical features of community-acquired or ventilator-associated
Ventilator-associated pneumonia (VAP) may complicate the course of bacterial pneumonia are indistinguishable from those described in the
HIV-infected patients who require mechanical ventilation. There is an immunocompetent host. Chest radiographs usually demonstrate seg-
increasing frequency of S aureus (methicillin-resistant S aureus [MRSA] mental or lobar consolidation.
or methicillin-sensitive S aureus [MSSA]) as a cause of VAP. In addition, Opportunistic infections and malignancies should be considered
aerobic gram-negative bacilli remain common causes of VAP. The other when the CD4 cell count is below 200 cells/mm although occasionally
3
diagnosis to consider in patients who have pulmonary infiltrates and who PJP may present at higher CD4 thresholds. Initial therapy for pneumo-
require mechanical ventilation is ventilator-associated lung injury. The nia should include broad-spectrum antimicrobial therapy and empiric
details of mechanical ventilation are discussed in Chaps. 48, 49, 51, and 52. influenza coverage should also be considered during winter. Empiric
coverage for PJP is not unreasonable if the radiographic findings are
supportive (see Fig. 69-1).
TABLE 69-3 Major Radiologic Differential Diagnosis of Lung Involvement in AIDS
Initial workup should include sputum culture and sensitivity for bac-
Normal chest x-ray PJP, MAC, MTb teria, fungi, and mycobacteria. Blood cultures should also be obtained,
Diffuse or localized interstitial pattern PJP, MTb, CMV, ALI/ARDS, cryptococcosis and in selected patients (ie, in those with advanced disease and CD4
cell counts below 50 or 100 cells/mm ), mycobacterial and fungal blood
3
Diffuse alveolar pattern PJP, viral pneumonia, cryptococcosis, cardiogenic cultures should be obtained. The key to diagnosis often requires suction
pulmonary edema, ALI/ARDS, VALI, ventilator- for tracheobronchial secretions. In the ICU setting, particularly in ven-
associated pneumonia
tilated patients, bronchoscopic bronchoalveolar lavage (BAL) is the pre-
Miliary pattern or reticulonodular MTb, histoplasmosis, coccidiodomycosis, ferred approach. Experienced specialists should perform BAL because
cryptococcosis critically ill patients with pneumonia are often at risk of complications
Consolidation Common bacteria, MTB, PJP, KS, ventilator- from bronchoscopy and BAL (such as hypoxemia and hypotension) and
associated pneumonia because of the need for care regarding the handling of specimens. In the
few patients for whom the initial BAL does not provide a diagnosis, a
Nodular opacity MTb, cryptococcosis, histoplasmosis, coccidioidomy-
cosis, common bacteria, KS, lymphoma, carcinoma transbronchial or open lung biopsy should be considered. However, the
appropriateness of such intervention is best decided on a case-by-case
Upper lung field involvement PJP, MTb basis after careful assessment of the general status of the patient, as well
Pneumothorax PJP, ventilator-associated barotrauma as the likelihood of diagnosing a treatable condition.
Cavity Bacteria, MTb, aspergillosis, histoplasmosis,
coccidioidomycosis, PJP PNEUMOCYSTIS JIROVECII PNEUMONIA
Pleural effusion Common bacteria, mycobacteria, KS Pneumocystis jirovecii (formerly carinii), recently reclassified as a fungus
ALI, acute lung injury; CMV, cytomegalovirus; KS, Kaposi sarcoma; MAC, Mycobacterium avium complex; MTb, but having some properties of protozoa, is a ubiquitous organism that
M tuberculosis; PJP, Pneumocystis jirovecii pneumonia; VALI, ventilator-associated lung injury. produces human disease throughout the world, usually in the setting of
section05_c61-73.indd 629 1/23/2015 12:48:15 PM