
Page 362 - Cardiac Nursing
P. 362
g
g
Pa
Pa
e 3
38
g
e 3
M
1
2:1
/09
1
6 A
M
2:1
6 A
38
a
In
ara
a
c.
c.
In
c.
ara
A
p
A
A
t
t
p
p
/09
3-3
33
33
3-3
q
87.
87.
p
LWB
LWBK340-c16_
LWB K34 0-c 16_ pp333-387.qxd 6/30/09 12:16 AM Page 338 Aptara Inc.
K34
p
16_
0-c
xd
/30
6
6
6
/30
q
q
xd
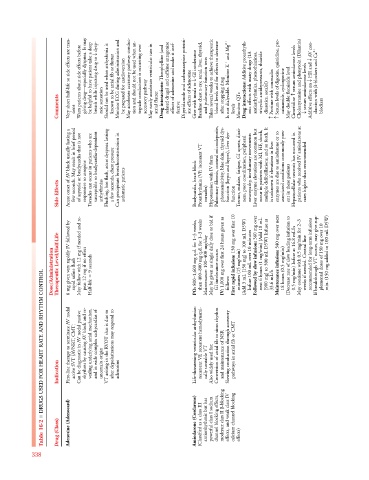
Very short half-life so side effects are tran- Warn patients about side effects before giving drug—especially dyspnea. It may be helpful to have patient take a deep dysp- breath while injecting drug to T Should not be used when arrhythmia is known to be atrial fib or flutter Monitor ECG during administration and be prepared for cardioversion May accelerate accessory pathway conduc- tion and should not be used when an- tegrade conduction is occurring over May rarely accelerate ventricular rate in Drug int
Comments sient neic sensation accessory pathway atrial flutter fective Give with meals to T after stopping drug levels Monitor QTc Drug interactions: diuretics, sotalol) c c May double flecainide level c Cimetidine T Additive effects on T blockers
Acute onset of AV block usually lasting a few seconds. May result in brief period of asystole or bradycardia that is not Torsades can occur in patients who are susceptible to bradycardia-dependent Flushing, hot flash, acute dyspnea lasting a few seconds, chest pressure Can precipitate bronchoconstriction in Proarrhythmia (VF, incessant VT, Pulmonary fibrosis, corneal microdeposits, photosensitivity, blue skin, thyroid dys- function (hypo and hyper), liver dys- Tremor, malaise, fatigue, GI upsets, dizzi-
Side Effects responsive to atropine arrhythmias asthmatic patients Bradycardia, heart block torsades) Hypotension with IV form function 360 mg over ent in these patients
Dose/Administration Therapeutic Level/Half-Life 6 mg given very rapidly IV followed by rapid saline flush May follow with 12 mg if needed and re- peat 12 mg if no effect 9 seconds Half-life 800–1,600 mg q.d. for 1–3 weeks, PO: then 400–800 mg q.d. for 1–3 weeks Maintenance: 100–400 mg/day May be given as single daily dose or bid if GI intolerance occurs 1,000 mg over first 24 hours given as IV: follows: 150 mg over first 10 First rapid infusion: minutes (15 mg/min) (Add 3 mL [150 mg] to 100 mL D5W) In
DRUGS USED FOR HEART RATE AND RHYTHM CONTROL
First-line therapy to terminate AV nodal active SVT (AVNRT, CMT) Can be diagnostic in AV nodal passive rhythms by causing AV block and re- vealing underlying atrial mechanism, and in wide complex tachycardias of VT arising in the RVOT that is due to after depolarizations may respond to Life-threatening ventricular arrhythmias: recurrent VF, recurrent hemodynami- Conversion of atrial fib to sinus rhythm and maintenance of NSR Slowing conduction through accessory pathways in atrial fib or CMT
Indication uncertain origin adenosine cally unstable VT Also widely used for:
■ Adenosine (Adenocard) Amiodarone (Cordarone) (Classified as a class III antiarrhythmic but has powerful class I sodium channel blocking effects, moderate class II -blocking effects, and weak class IV calcium channel blocking
Table 16-2 Drug (Class) effects)
338