
Page 367 - Cardiac Nursing
P. 367
g
g
Pa
g
43
43
e 3
e 3
2:1
6 A
1
2:1
M
Pa
6 A
M
A
a
In
ara
a
c.
c.
In
c.
p
p
A
A
t
ara
p
t
1
33
33
p
87.
3-3
3-3
16_
K34
K34
LWBK340-c16_ p pp333-387.qxd 6/30/09 12:16 AM Page 343 Aptara Inc.
16_
0-c
0-c
6
6
xd
q
xd
/09
/09
/30
6
/30
q
q
87.
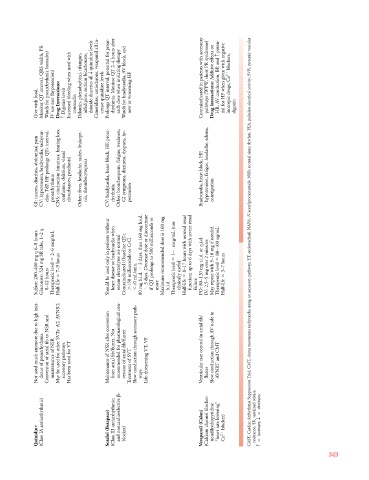
Monitor QT interval, QRS width, PR Watch for proarrhythmia (torsades) Increased bleeding when used with Dilantin, phenobarbital, rifampin, nifedipine, sodium bicarbonate, quinidine levels Cimetidine, amiodarone, verapamil all in- Prolongs QT interval, potential for proar- rhythmia. Monitor QT 2–4 hours after each dose when initiating therapy Watch for bradycardia, AV block, and Contraindicated in patients with accessory pathways (WPW, short PR syndrome) Additive effects on poten- HR, AV conduction, BP , and
Give with food. IV use rare (hypotension) Drug Interactions: Digoxin levels c coumadin thiazide diuretics all T crease quinidine levels new or worsening HF Drug interactions: digoxin
GI: nausea, diarrhea, abdominal pain CV: hypotension, bradycardia, tachycar- dias, TdP , HF prolongs QTc interval, proarrhythmia CNS: cinchonism (tinnitus, hearing loss, confusion, delirium, visual disturbances, psychosis) Other: fever, headache, rashes, leukope- nia, thrombocytopenia CV: bradycardia, heart block, HF, proar- rhythmia Other: bronchospasm, fatigue, weakness, GI symptoms, dizziness, dyspnea, hy- potension Bradycardia, heart block, HF, hypotension, fatigue, headache, edema, constipation N N
Sulfate: 200–400 mg q 6–8 hours Gluconate: 324 mg SR tabs, 1–2 q 8–12 hours 2–6 mcg/mL Therapeutic level 7–9 hours Half-life Should be used only in patients without heart disease or bradycardia when serum electrolytes are normal Contraindicated if baseline QTc 450 milliseconds or CrCl 40 mL/min. 3 days, then 160 mg b.i.d. 80 mg b.i.d. 3 days. Decrease dose or discontinue if QT prolongs to 500 milliseconds or more Maximum recommended dose is 160 mg b.i.d 1–4 mcg/mL (not Therapeutic level c
Not used much anymore due to high inci- dence of proarrhythmia Conversion of atrial fib to NSR and maintenance of NSR May be used for other SVTs: AT, AVNRT, accessory pathways Has been used for VT Maintenance of NSR after conversion from atrial fib/flutter. Not recommended for pharmacological con- version of atrial fib/flutter Treatment of SVT Slow conduction through accessory path- Life-threatening VT, VF Ventricular rate control in atrial fib/ Slow conduction through AV node in AVNRT and CMT
- ways flutter decreases.
(Class IA antiarrhythmic) Sotalol (Betapace) (Class III antiarrhythmic; and noncardioselective Verapamil (Calan) (Calcium channel blocker: nondihydropyridine “heart rate lowering” blocker) resistance, SR, sustained release. increases, T
Quinidine blocker) Ca 2
c
343