
Page 44 - Cardiac Nursing
P. 44
92806_c01.qxd 11/21/11 10:30 AM Page 20
20 PA R T I / Anatomy and Physiology
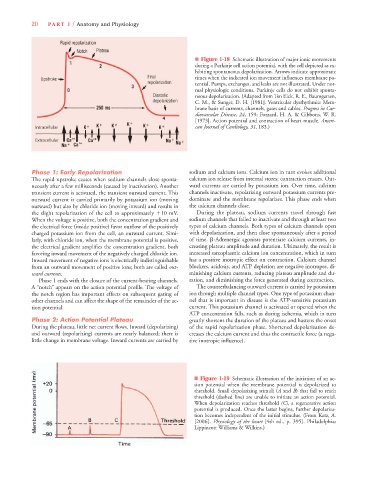
■ Figure 1-18 Schematic illustration of major ionic movements
during a Purkinje cell action potential, with the cell depicted as ex-
hibiting spontaneous depolarization. Arrows indicate approximate
times when the indicated ion movement influences membrane po-
tential. Pumps, exchanges, and leaks are not illustrated. Under nor-
mal physiologic conditions, Purkinje cells do not exhibit sponta-
neous depolarization. (Adapted from Ten Eick, R. E., Baumgarten,
C. M., & Sunger, D. H. [1981]. Ventricular dysrhythmia: Mem-
brane basis of currents, channels, gates and cables. Progress in Car-
diovascular Disease, 24, 159; Fozzard, H. A. & Gibbons, W. R.
[1973]. Action potential and contraction of heart muscle. Ameri-
can Journal of Cardiology, 31, 183.)
Phase 1: Early Repolarization sodium and calcium ions. Calcium ion in turn evokes additional
The rapid upstroke ceases when sodium channels close sponta- calcium ion release from internal stores; contraction ensues. Out-
neously after a few milliseconds (caused by inactivation). Another ward currents are carried by potassium ion. Over time, calcium
transient current is activated, the transient outward current. This channels inactivate, repolarizing outward potassium currents pre-
outward current is carried primarily by potassium ion (moving dominate and the membrane repolarizes. This phase ends when
outward) but also by chloride ion (moving inward) and results in the calcium channels close.
the slight repolarization of the cell to approximately 10 mV. During the plateau, sodium currents travel through fast
When the voltage is positive, both the concentration gradient and sodium channels that failed to inactivate and through at least two
the electrical force (inside positive) favor outflow of the positively types of calcium channels. Both types of calcium channels open
charged potassium ion from the cell, an outward current. Simi- with depolarization, and then close spontaneously after a period
larly, with chloride ion, when the membrane potential is positive, of time. -Adrenergic agonists potentiate calcium currents, in-
the electrical gradient amplifies the concentration gradient, both creasing plateau amplitude and duration. Ultimately, the result is
favoring inward movement of the negatively charged chloride ion. increased sarcoplasmic calcium ion concentration, which in turn
Inward movement of negative ions is electrically indistinguishable has a positive inotropic effect on contraction. Calcium channel
from an outward movement of positive ions; both are called out- blockers, acidosis, and ATP depletion are negative inotropes, di-
ward currents. minishing calcium currents, reducing plateau amplitude and du-
Phase 1 ends with the closure of the current-bearing channels. ration, and diminishing the force generated during contraction.
A “notch” appears on the action potential profile. The voltage of The counterbalancing outward current is carried by potassium
the notch region has important effects on subsequent gating of ion through multiple channel types. One type of potassium chan-
other channels and can affect the shape of the remainder of the ac- nel that is important in disease is the ATP-sensitive potassium
tion potential. current. This potassium channel is activated or opened when the
ATP concentration falls, such as during ischemia, which in turn
Phase 2: Action Potential Plateau greatly shortens the duration of the plateau and hastens the onset
During the plateau, little net current flows. Inward (depolarizing) of the rapid repolarization phase. Shortened depolarization de-
and outward (repolarizing) currents are nearly balanced; there is creases the calcium current and thus the contractile force (a nega-
little change in membrane voltage. Inward currents are carried by tive inotropic influence).
■ Figure 1-19 Schematic illustration of the initiation of an ac-
tion potential when the membrane potential is depolarized to
threshold. Small depolarizing stimuli (A and B) that fail to reach
threshold (dashed line) are unable to initiate an action potential.
When depolarization reaches threshold (C), a regenerative action
potential is produced. Once the latter begins, further depolariza-
tion becomes independent of the initial stimulus. (From Katz, A.
[2006]. Physiology of the heart [4th ed., p. 395]. Philadelphia:
Lippincott Williams & Wilkins.)