
Page 446 - Cardiac Nursing
P. 446
7 A
p42
e 4
0-4
0
9/2
009
22
9/0
Apt
22
38.
P
qxd
38.
g
ara
P
M
LWBK340-c19_19_p420-438.qxd 09/09/2009 08:27 AM Page 422 Aptara
L L LWB
19_
K34
K34
LWB K34 0-c 19_ p42 0-4 38. qxd 0 9/0 9/2 009 0 0 8:2 7 A M P a a g e 4 22 Apt ara
8:2
0-c
422 P A R T III / Assessment of Heart Disease
Table 19-1 ■ COMMON DRUGS AND THEIR IMPACT ON EXERCISE TESTING
Drug Indications Heart Rate Blood Pressure Electrocardiogram Exercise Capacity
-Blockers Angina, hypertension, Rest: ↓, exercise: ↓ Rest: ↓, exercise: ↓ ↓ Signs of ischemia ↑ In those with angina,
MI, arrhythmias, ↓ in those without
tremors, migraine angina
headache
Calcium channel Angina, coronary artery Rest: ↓, exercise: ↓ Rest: ↓, exercise: ↓ ↓ Signs of ischemia ↑ In those with angina,
blockers spasm, hypertension minimal effect in
those without angina
Digoxin CHF, arrhythmias No change Rest: ↓, Exercise: ↓ Will cause false-positive ↑ In those with CHF
responses
Nitrates Angina No change Rest: ↓, Exercise: ↓ Delayed signs of ischemia ↑ In those with angina
(and CHF)
abraded using an abrasive pad or other product designed for this For this reason, diagnostic ST-segment changes should always be
purpose. Finally, each electrode should be carefully placed in the made relative to the resting baseline position (i.e., upright rather
proper location to ensure good skin contact with both the con- than supine position for treadmill and cycle ergometry).
ducting gel and adhesive surfaces of the electrode.
18
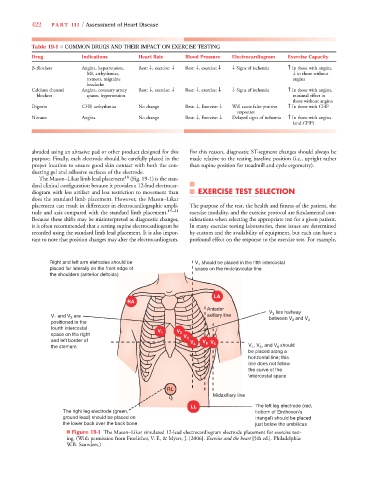
The Mason–Likar limb lead placement (Fig. 19-1) is the stan-
dard clinical configuration because it provides a 12-lead electrocar-
diogram with less artifact and less restriction to movement than EXERCISE TEST SELECTION
does the standard limb placement. However, the Mason–Likar
placement can result in differences in electrocardiographic ampli- The purpose of the test, the health and fitness of the patient, the
tude and axis compared with the standard limb placement. 19–21 exercise modality, and the exercise protocol are fundamental con-
Because these shifts may be misinterpreted as diagnostic changes, siderations when selecting the appropriate test for a given patient.
it is often recommended that a resting supine electrocardiogram be In many exercise testing laboratories, these issues are determined
recorded using the standard limb lead placement. It is also impor- by custom and the availability of equipment, but each can have a
tant to note that position changes may alter the electrocardiogram. profound effect on the response to the exercise test. For example,
Right and left arm eletrodes should be V should be placed in the fifth intercostal
4
placed far laterally on the front edge of space on the midclavicular line
the shoulders (anterior deltoids))
LA
RA
Anterior
A A o V lies halfway
3
ry
lla
V and V are axiillary y y line between V and V
1
2
positioned in the 2 4
fourth intercostal
V 1 V 2
space on the right
V 3
and left border of
5
V 4 V V 6
the stemum V , V , and V should
4
6
5
be placed along a
horizontal line; this
line does not follow
the curve ot the
\intercostal space
RL
Mid daxillary lin ne
LL The left leg electrode (red,
The right leg electrode (green, bottom of Einthoven’s
ground lead) should be placed on triangel) should be placed
the lower back over the back bone just below the umbilicus
■ Figure 19-1 The Mason–Likar simulated 12-lead electrocardiogram electrode placement for exercise test-
ing. (With permission from Froelicher, V. F., & Myers, J. [2006]. Exercise and the heart [5th ed.]. Philadelphia:
W.B. Saunders.)