
Page 450 - Cardiac Nursing
P. 450
LWBK340-c19_p420-438.qxd 09/09/2009 08:27 AM Page 426 Aptara
426 PA R T III / Assessment of Heart Disease
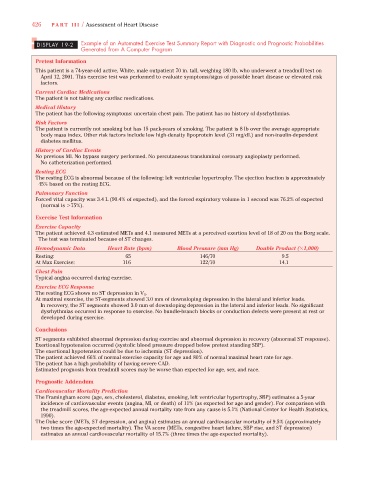
DISPLAY 19-2 Example of an Automated Exercise Test Summary Report with Diagnostic and Prognostic Probabilities
Generated from A Computer Program
Pretest Information
This patient is a 74-year-old active, White, male outpatient 70 in. tall, weighing 180 lb, who underwent a treadmill test on
April 12, 2001. This exercise test was performed to evaluate symptoms/signs of possible heart disease or elevated risk
factors.
Current Cardiac Medications
The patient is not taking any cardiac medications.
Medical History
The patient has the following symptoms: uncertain chest pain. The patient has no history of dysrhythmias.
Risk Factors
The patient is currently not smoking but has 15 pack-years of smoking. The patient is 8 lb over the average appropriate
body mass index. Other risk factors include low high-density lipoprotein level (31 mg/dL) and non-insulin-dependent
diabetes mellitus.
History of Cardiac Events
No previous MI. No bypass surgery performed. No percutaneous transluminal coronary angioplasty performed.
No catheterization performed.
Resting ECG
The resting ECG is abnormal because of the following: left ventricular hypertrophy. The ejection fraction is approximately
45% based on the resting ECG.
Pulmonary Function
Forced vital capacity was 3.4 L (90.4% of expected), and the forced expiratory volume in 1 second was 76.2% of expected
(normal is 75%).
Exercise Test Information
Exercise Capacity
The patient achieved 4.3 estimated METs and 4.1 measured METs at a perceived exertion level of 18 of 20 on the Borg scale.
The test was terminated because of ST changes.
(
Hemodynamic Data Heart Rate (bpm) Blood Pressure (mm Hg) Double Product ( 1,000)
(
Resting: 65 146/70 9.5
At Max Exercise: 116 122/70 14.1
Chest Pain
Typical angina occurred during exercise.
Exercise ECG Response
The resting ECG shows no ST depression in V 5 .
At maximal exercise, the ST-segments showed 3.0 mm of downsloping depression in the lateral and inferior leads.
In recovery, the ST segments showed 3.0 mm of downsloping depression in the lateral and inferior leads. No significant
dysrhythmias occurred in response to exercise. No bundle-branch blocks or conduction defects were present at rest or
developed during exercise.
Conclusions
ST segments exhibited abnormal depression during exercise and abnormal depression in recovery (abnormal ST response).
Exertional hypotension occurred (systolic blood pressure dropped below pretest standing SBP).
The exertional hypotension could be due to ischemia (ST depression).
The patient achieved 66% of normal exercise capacity for age and 80% of normal maximal heart rate for age.
The patient has a high probability of having severe CAD.
Estimated prognosis from treadmill scores may be worse than expected for age, sex, and race.
Prognostic Addendum
Cardiovascular Mortality Prediction
The Framingham score (age, sex, cholesterol, diabetes, smoking, left ventricular hypertrophy, SBP) estimates a 5-year
incidence of cardiovascular events (angina, MI, or death) of 11% (as expected for age and gender). For comparison with
the treadmill scores, the age-expected annual mortality rate from any cause is 5.1% (National Center for Health Statistics,
1990).
The Duke score (METs, ST depression, and angina) estimates an annual cardiovascular mortality of 9.5% (approximately
two times the age-expected mortality). The VA score (METs, congestive heart failure, SBP rise, and ST depression)
estimates an annual cardiovascular mortality of 15.7% (three times the age-expected mortality).