
Page 763 - Cardiac Nursing
P. 763
CHAPTER 31 / Adult Congenital Heart Disease 739
n Figure 31-1 Categorization of congenital heart defects.
and presence of increased pulmonary vascular disease. Adults with pulmonary resistance exceeds systemic pressure, patients are ren-
small left-to-right shunts from a persistent ductus have no symp- dered inoperable.
toms and life expectancy is normal. Patients with large shunts
and relatively low pulmonary vascular resistance are at risk for Clinical Manifestations
developing left ventricular failure, pulmonary vascular disease, The clinical appearance characterizing a moderate or large PDA
and reversed shunting. In such cases, operation is advised. Once with normal pulmonary arterial pressure includes bounding pe-
ripheral pulses, a widened pulse pressure, with diastolic pressures
as low as 30 to 50 mm Hg. The left ventricular impulse is hyper-
dynamic, and, if present, a systolic thrill may be palpated over the
suprasternal notch area. A continuous loud “machinery” murmur
accentuated in late systole is heard best in the first or second left
intercostal space. In the setting of increased pulmonary vascular
resistance, the diastolic component of the murmur disappears,
leaving only the systolic component.
Patients with a moderate shunt may have no symptoms during
infancy but may begin to develop fatigue, dyspnea, or palpitations
during childhood or adulthood. Occasionally, the ductus arterio-
sus may become aneurismal, calcified, and rupture. 13
Management
In the absence of pulmonary vascular disease, it is recommended
that all PDAs be closed either by surgical ligation or by interven-
tional catheterization using percutaneous closure devices. Patients
with moderate to large size PDAs who go unrepaired are at risk for
endarteritis, heart failure, and pulmonary hypertension. One third
of these patients die by the age of 40 years; two thirds of them die
by the age of 60 year. 13,19 Once closed, periodic long-term evalua-
tion is recommended because residual problems such as pulmonary
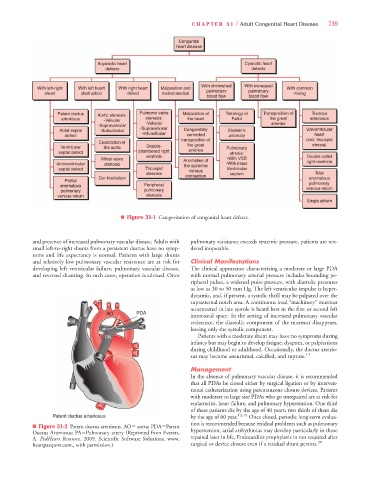
n Figure 31-2 Patent ductus arteriosus. AO5 aorta; PDA5Patent
Ductus Arteriosus; PA5Pulmonary artery (Reprinted from Everett, hypertension, atrial arrhythmias may develop particularly in those
A. PedHeart Resource. 2009. Scientific Software Solutions. www. repaired later in life. Endocarditis prophylaxis in not required after
20
heartpassport.com., with permission.) surgical or device closure even if a residual shunt persists.