
Page 764 - Cardiac Nursing
P. 764
740 P AR T IV / Pathophysiology and Management of Heart Disease
vascular bed. In infancy, the persistence of increased pulmonary
vascular resistance and the relatively equally compliant left and
right ventricles limit the amount of left-to-right shunting. With
increasing age, pulmonary vascular resistance decreases, and the
right ventricle becomes thinner, offering less resistance to filling
than the left. Consequently, the conditions are appropriate for
left-to-right flow across the defect. Although left atrial pressure is
only slightly higher than right atrial pressure, a left-to-right shunt
is present, and the pulmonary blood flow may exceed systemic
blood flow by three to four times. 21
Major problems of adults with unrepaired ASD include the
development of atrial arrhythmias, which increase in frequency
with age; a persistent rise in pulmonary vascular resistance leading
eventually to reversed shunting and cyanosis, or the Eisenmenger
reaction; and heart failure. The latter is usually the result of asso-
ciated diseases affecting left ventricular function, such as systemic
hypertension or ischemic heart disease. Left ventricular failure re-
duces the distensibility of the left ventricle, increasing the volume
of left atrial blood being shunted across the defect, thus adding to
n Figure 31-3 Atrial septal defect. (Reprinted from Everett, A.
PedHeart Resource. 2009. Scientific Software Solutions. www.heart the burden of an already volume-overloaded right ventricle.
passport.com., with permission.)
Clinical Manifestations
Characteristic of the increased pulmonary flow across the pul-
monic valves is a soft mid-systolic pulmonic ejection murmur. If
Atrial Septal Defects the shunt is large, a mild diastolic rumbling murmur is heard at
the lower left sternal border, due to increased blood flow across
Description the tricuspid valve. A second sound, which is widely split and does
Atrial septal defects (ASDs) are abnormal communications not vary with respiration, is consistent with a low pulmonary vas-
between the left and right atria (Fig. 31-3). They constitute 10% cular resistance. Prominent right ventricle pulsations along the left
of all congenital heart anomalies. There is a female predomi- sternal border and pulmonary artery are palpable. The presence of
nance. 14 They are differentiated by their occurrence within the a systolic thrill reflects a large shunt or coexisting pulmonic steno-
septum. Ostium secundum ASD, the most common type, occurs sis. In ostium primum, there is the addition of the murmur of mi-
in the central region of the fossa ovalis. Ostium primum ASD, tral regurgitation, a left ventricular impulse, and systolic thrill. In
which occurs low in the atrial septum, has an associated cleft an- sinus venosus, the clinical findings are similar to the ostium se-
terior mitral valve with varying degree of mitral insufficiency. Sinus cundum. Most patients with ASD remain asymptomatic but may
venosus ASD occurs in the upper part of the atrial septum near the complain of easy fatigability and exertional dyspnea.
entry of the superior vena cava and may be associated with the par-
tial anomalous right pulmonary venous connection (Fig. 31-4). Management
Owing to the trivial or absent physical signs, ASD may go unde- Closure of ASD is recommended if the pulmonary-to-systemic blood
tected until the fourth or fifth decade. flow ratio (Q p /Q s ) is $1.5:1. Most surgical repairs are performed
in infancy by simple suture closure; in larger defects a pericardial
Pathophysiology or prosthetic patch may be required to close the defect. For Ostium
The hemodynamic consequences of ASD are dependent on (1) the primum defects, repair of the mitral valve cleft is also undertaken.
size and direction of the shunt; (2) the compliance of the left and If mitral insufficiency persists, the patient must be followed closely
right ventricles; and (3) the responsive behavior of the pulmonary to determine need for further valve repair or even replacement.
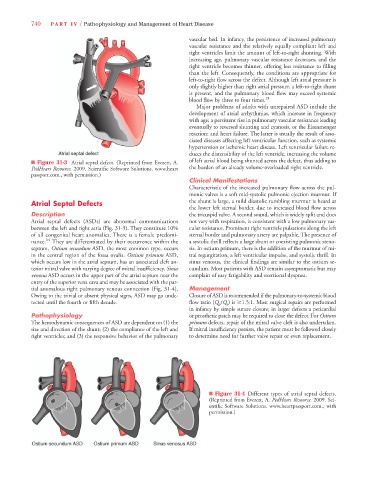
n Figure 31-4 Different types of atrial septal defects.
(Reprinted from Everett, A. PedHeart Resource. 2009. Sci-
entific Software Solutions. www.heartpassport.com., with
permission.)