
Page 784 - Cardiac Nursing
P. 784
1
2:0
4 A
009
009
1
A
A
A
A
A
A
d
3
0
3-7
68.
qx
0
6
2
p7
0
/
ara
LWB K34 0-c 32_ p7 5 3-7 68. qx d 3 0 / 0 6 / / 2 009 1 2:0 4 A M Pa g g e 7 60 Apt ara
Apt
ara
L L LWB
0-c
K34
LWBK340-c32_32_p7553-768.qxd 30/06/2009 12:04 AM Page 760 Aptara
32_
A
M
A
A
A
Pa
e 7
60
60
760 PA R T V / Health Promotion and Disease Prevention
9
8
7
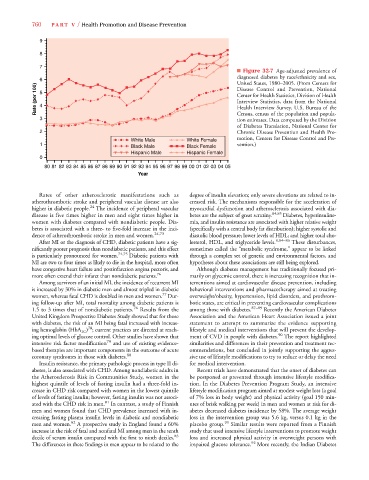
■ Figure 32-7 Age-adjusted prevalence of
diagnosed diabetes by race/ethnicity and sex,
6 United States, 1980–2005. (From Centers for
Rate (per 100) 5 4 Disease Control and Prevention, National
Center for Health Statistics, Division of Health
Interview Statistics, data from the National
Health Interview Survey. U.S. Bureau of the
3 Census, census of the population and popula-
tion estimates. Data computed by the Division
of Diabetes Translation, National Center for
2 Chronic Disease Prevention and Health Pro-
White Male White Female motion, Centers for Disease Control and Pre-
1 Black Male Black Female vention.)
Hispanic Male Hispanic Female
0
80 81828384858687888990919293 949596979899000102030405
Year
Rates of other atherosclerotic manifestations such as degree of insulin elevation; only severe elevations are related to in-
atherothrombotic stroke and peripheral vascular disease are also creased risk. The mechanisms responsible for the acceleration of
higher in diabetic people. 24 The incidence of peripheral vascular myocardial dysfunction and atherosclerosis associated with dia-
disease is five times higher in men and eight times higher in betes are the subject of great scrutiny. 84,85 Diabetes, hyperinsuline-
women with diabetes compared with nondiabetic people. Dia- mia, and insulin resistance are associated with higher relative weight
betes is associated with a three- to five-fold increase in the inci- (specifically with a central body fat distribution); higher systolic and
dence of atherothrombotic stroke in men and women. 24,73 diastolic blood pressure; lower levels of HDL; and higher total cho-
After MI or the diagnosis of CHD, diabetic patients have a sig- lesterol, HDL, and triglyceride levels. 8,84–86 These disturbances,
nificantly poorer prognosis than nondiabetic patients, and this effect sometimes called the “metabolic syndrome,” appear to be linked
is particularly pronounced for women. 74,75 Diabetic patients with through a complex set of genetic and environmental factors, and
MI are two to four times as likely to die in the hospital, more often hypotheses about these associations are still being explored.
have congestive heart failure and postinfarction angina pectoris, and Although diabetes management has traditionally focused pri-
more often extend their infarct than nondiabetic patients. 76 marily on glycemic control, there is increasing recognition that in-
Among survivors of an initial MI, the incidence of recurrent MI terventions aimed at cardiovascular disease prevention, including
is increased by 30% in diabetic men and almost tripled in diabetic behavioral interventions and pharmacotherapy aimed at treating
77
women, whereas fatal CHD is doubled in men and women. Dur- overweight/obesity, hypertension, lipid disorders, and prothrom-
ing follow-up after MI, total mortality among diabetic patients is botic states, are critical in preventing cardiovascular complications
1.5 to 3 times that of nondiabetic patients. 76 Results from the among those with diabetes. 87–89 Recently the American Diabetes
United Kingdom Prospective Diabetes Study showed that for those Association and the American Heart Association issued a joint
with diabetes, the risk of an MI being fatal increased with increas- statement to attempt to summarize the evidence supporting
78
ing hemoglobin (HbA 1C ) ; current practices are directed at reach- lifestyle and medical interventions that will prevent the develop-
ing optimal levels of glucose control. Other studies have shown that ment of CVD in people with diabetes. 90 The report highlighted
intensive risk factor modification 79 and use of existing evidence- similarities and differences in their prevention and treatment rec-
based therapies are important components in the outcome of acute ommendations, but concluded in jointly supporting the aggres-
coronary syndromes in those with diabetes. 80 sive use of lifestyle modifications to try to reduce or delay the need
Insulin resistance, the primary pathologic process in type II di- for medical intervention.
abetes, is also associated with CHD. Among nondiabetic adults in Recent trials have demonstrated that the onset of diabetes can
the Atherosclerosis Risk in Communities Study, women in the be postponed or prevented through intensive lifestyle modifica-
highest quintile of levels of fasting insulin had a three-fold in- tion. In the Diabetes Prevention Program Study, an intensive
crease in CHD risk compared with women in the lowest quintile lifestyle modification program aimed at modest weight loss (a goal
of levels of fasting insulin; however, fasting insulin was not associ- of 7% loss in body weight) and physical activity (goal 150 min-
ated with the CHD risk in men. 81 In contrast, a study of Finnish utes of brisk walking per week) in men and women at risk for di-
men and women found that CHD prevalence increased with in- abetes decreased diabetes incidence by 58%. The average weight
creasing fasting plasma insulin levels in diabetic and nondiabetic loss in the intervention group was 5.6 kg, versus 0.1 kg in the
men and women. 82 A prospective study in England found a 60% placebo group. 91 Similar results were reported from a Finnish
increase in the risk of fatal and nonfatal MI among men in the tenth study that used intensive lifestyle interventions to promote weight
decile of serum insulin compared with the first to ninth deciles. 83 loss and increased physical activity in overweight persons with
92
The differences in these findings in men appear to be related to the impaired glucose tolerance. More recently, the Indian Diabetes