
Page 800 - Cardiac Nursing
P. 800
8:3
8:3
5 A
0
009
009
0
P
P
a
P
5 A
M
M
9/2
82.
82.
82.
qxd
0
0
qxd
p76
p76
9/2
9/0
9-7
9-7
9/0
L L LWB
K34
LWB
ara
LWBK340-c33_33_p769-782.qxd 09/09/2009 08:35 AM Page 776 Aptara
33_
0-c
K34
K34
33_
0-c
ara
e 7
a
e 7
g
g
76
Apt
Apt
76
76
776 PA R T V / Health Promotion and Disease Prevention
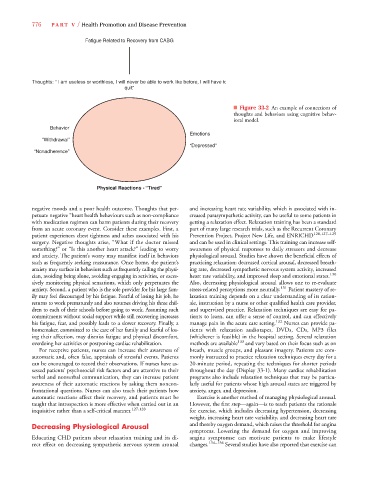
Fatigue Related to Recovery from CABG
Thoughts: “ I am useless or worthless, I will never be able to work like before, I will have to
quit”
■ Figure 33-2 An example of connections of
thoughts and behaviors using cognitive behav-
ioral model.
Behavior
Emotions
“Withdrawal”
“Depressed”
“Nonadherence”
Physical Reactions - “Tired”
negative moods and a poor health outcome. Thoughts that per- and increasing heart rate variability, which is associated with in-
petuate negative “heart health behaviours such as non-compliance creased parasympathetic activity, can be useful to some patients in
with medication regimen can harm patients during their recovery getting a relaxation effect. Relaxation training has been a standard
from an acute coronary event. Consider these examples. First, a part of many large research trials, such as the Recurrent Coronary
patient experiences chest tightness and aches associated with his Prevention Project, Project New Life, and ENRICHD 120,127–129
surgery. Negative thoughts arise, “What if the doctor missed and can be used in clinical settings. This training can increase self-
something?” or “Is this another heart attack?” leading to worry awareness of physical responses to daily stressors and decrease
and anxiety. The patient’s worry may manifest itself in behaviors physiological arousal. Studies have shown the beneficial effects of
such as frequently seeking reassurance. Once home, the patient’s practicing relaxation: decreased cortical arousal, decreased breath-
anxiety may surface in behaviors such as frequently calling the physi- ing rate, decreased sympathetic nervous system activity, increased
cian, avoiding being alone, avoiding engaging in activities, or exces- heart rate variability, and improved sleep and emotional states. 130
sively monitoring physical sensations, which only perpetuates the Also, decreasing physiological arousal allows one to re-evaluate
anxiety. Second, a patient who is the sole provider for his large fam- stress-related perceptions more neutrally. 131 Patient mastery of re-
ily may feel discouraged by his fatigue. Fearful of losing his job, he laxation training depends on a clear understanding of its ration-
returns to work prematurely and also resumes driving his three chil- ale, instruction by a nurse or other qualified health care provider,
dren to each of their schools before going to work. Assuming such and supervised practice. Relaxation techniques are easy for pa-
commitments without social support while still recovering increases tients to learn, can offer a sense of control, and can effectively
his fatigue, fear, and possibly leads to a slower recovery. Finally, a manage pain in the acute care setting. 132 Nurses can provide pa-
homemaker, committed to the care of her family and fearful of los- tients with relaxation audiotapes, DVDs, CDs, MP3 files
ing their affection, may dismiss fatigue and physical discomfort, (whichever is feasible) in the hospital setting. Several relaxation
overdoing her activities or postponing cardiac rehabilitation. methods are available 133 and vary based on their focus such as on
For receptive patients, nurses can increase their awareness of breath, muscle groups, and pleasant imagery. Patients are com-
automatic and, often false, appraisals of stressful events. Patients monly instructed to practice relaxation techniques every day for a
can be encouraged to record their observations. If nurses have as- 20-minute period, repeating the techniques for shorter periods
sessed patients’ psychosocial risk factors and are attentive to their throughout the day (Display 33-1). Many cardiac rehabilitation
verbal and nonverbal communication, they can increase patient programs also include relaxation techniques that may be particu-
awareness of their automatic reactions by asking them noncon- larly useful for patients whose high arousal states are triggered by
frontational questions. Nurses can also teach their patients how anxiety, anger, and depression.
automatic reactions affect their recovery, and patients must be Exercise is another method of managing physiological arousal.
taught that introspection is more effective when carried out in an However, the first step—again—is to teach patients the rationale
inquisitive rather than a self-critical manner. 127,128 for exercise, which includes decreasing hypertension, decreasing
weight, increasing heart rate variability, and decreasing heart rate
Decreasing Physiological Arousal and thereby oxygen demand, which raises the threshold for angina
symptoms. Lowering the demand for oxygen and improving
Educating CHD patients about relaxation training and its di- angina symptomse can motivate patients to make lifestyle
rect effect on decreasing sympathetic nervous system arousal changes. 134–136 Several studies have also reported that exercise can