
Page 477 - ACCCN's Critical Care Nursing
P. 477
454 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
50
significant reduction in ICP for both TBI and ischaemic cerebral vasospasm occurs in approximately 10–15%
51
stroke. In 2011 a multi-centre prospective randomised of patients.
trial of early decompressive craniectomy in patients with
severe traumatic brain injury reported that in adults Calcium antagonists, such as nimodipine, have not been
with severe diffuse traumatic brain injury and refractory effective in TBI subarachnoid haemorrhage with vaso-
intracranial hypertension, early bifrontotemporoparietal spasm, and recent studies have suggested that calcium
decompressive craniectomy decreased intracranial pres- antagonists even prevent neurogenesis after TBI. Nimo-
sure and the length of stay in the ICU but surprisingly dipine has demonstrated effectiveness in the treatment of
was associated with more unfavorable outcomes at both vasospasm in aneurysmal SAH and is now an option for
6 and 12 months using the Extended Glasgow Outcome recommended practice. An initial study of nimodipine in
Scale. 52 patients with TBI demonstrated no difference in out-
come, and a Cochrane Systematic Review supports this
Prevention of Cerebral Vasospasm conclusion. 53
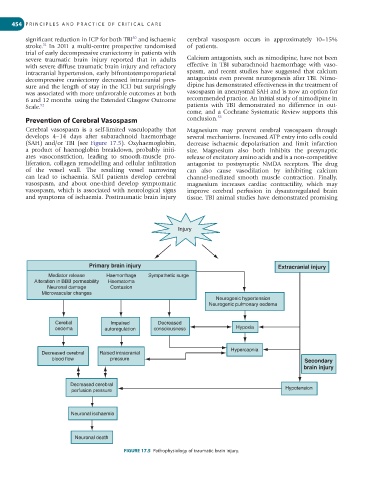
Cerebral vasospasm is a self-limited vasculopathy that Magnesium may prevent cerebral vasospasm through
develops 4–14 days after subarachnoid haemorrhage several mechanisms. Increased ATP entry into cells could
(SAH) and/or TBI (see Figure 17.5). Oxyhaemoglobin, decrease ischaemic depolarisation and limit infarction
a product of haemoglobin breakdown, probably initi- size. Magnesium also both inhibits the presynaptic
ates vasoconstriction, leading to smooth-muscle pro- release of excitatory amino acids and is a non-competitive
liferation, collagen remodelling and cellular infiltration antagonist to postsynaptic NMDA receptors. The drug
of the vessel wall. The resulting vessel narrowing can also cause vasodilation by inhibiting calcium
can lead to ischaemia. SAH patients develop cerebral channel-mediated smooth muscle contraction. Finally,
va sospasm, and about one-third develop symptomatic magnesium increases cardiac contractility, which may
vasospasm, which is associated with neurological signs improve cerebral perfusion in dysautoregulated brain
and symptoms of ischaemia. Posttraumatic brain injury tissue. TBI animal studies have demonstrated promising
Injury
Primary brain injury Extracranial injury
Mediator release Haemorrhage Sympathetic surge
Alteration in BBB permeability Haematoma
Neuronal damage Contusion
Microvascular changes
Neurogenic hypertension
Neurogenic pulmonary oedema
Cerebal Impaired Decreased
oedema autoregulation consciousness Hypoxia
Hypercapnia
Decreased cerebral Raised intracranial
blood flow pressure Secondary
brain injury
Decreased cerebral
perfusion pressure Hypotension
Neuronal ischaemia
Neuronal death
FIGURE 17.5 Pathophysiology of traumatic brain injury.