
Page 570 - ACCCN's Critical Care Nursing
P. 570
Management of Shock 547
Systolic dysfunction
stroke volume, ejection fraction
Blood pressure Cardiac output
Sympathoadrenal activation
(compensation)
Heart rate Inotropy Systemic
vascular resistance
Myocardial oxygen demands
(± ischaemia)
Congestion
left ventricular end-diastolic volume and pressure
left atrial pressue
global end-diastolic volume index
pulmonary capillary wedge pressure
pulmonary artery pressure
extravascular lung water index
intrathoracic blood volume index
right ventricular systolic/diastolic pressure
right atrial pressure
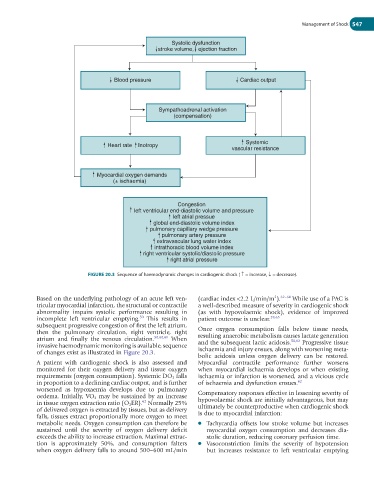
FIGURE 20.3 Sequence of haemodynamic changes in cardiogenic shock ( ↑ = increase, ↓ = decrease).
Based on the underlying pathology of an acute left ven- (cardiac index <2.2 L/min/m ). 62–64 While use of a PAC is
2
tricular myocardial infarction, the structural or contractile a well-described measure of severity in cardiogenic shock
abnormality impairs systolic performance resulting in (as with hypovolaemic shock), evidence of improved
incomplete left ventricular emptying. This results in patient outcome is unclear. 28,65
50
subsequent progressive congestion of first the left atrium,
then the pulmonary circulation, right ventricle, right Once oxygen consumption falls below tissue needs,
atrium and finally the venous circulation. 50,60,61 When resulting anaerobic metabolism causes lactate generation
50,62
invasive haemodynamic monitoring is available, sequence and the subsequent lactic acidosis. Progressive tissue
of changes exist as illustrated in Figure 20.3. ischaemia and injury ensues, along with worsening meta-
bolic acidosis unless oxygen delivery can be restored.
A patient with cardiogenic shock is also assessed and Myocardial contractile performance further worsens
monitored for their oxygen delivery and tissue oxygen when myocardial ischaemia develops or when existing
requirements (oxygen consumption). Systemic DO 2 falls ischaemia or infarction is worsened, and a vicious cycle
in proportion to a declining cardiac output, and is further of ischaemia and dysfunction ensues. 62
worsened as hypoxaemia develops due to pulmonary Compensatory responses effective in lessening severity of
oedema. Initially, VO 2 may be sustained by an increase hypovolaemic shock are initially advantageous, but may
62
in tissue oxygen extraction ratio (O 2ER). Normally 25% ultimately be counterproductive when cardiogenic shock
of delivered oxygen is extracted by tissues, but as delivery is due to myocardial infarction:
falls, tissues extract proportionally more oxygen to meet
metabolic needs. Oxygen consumption can therefore be ● Tachycardia offsets low stroke volume but increases
sustained until the severity of oxygen delivery deficit myocardial oxygen consumption and decreases dia-
exceeds the ability to increase extraction. Maximal extrac- stolic duration, reducing coronary perfusion time.
tion is approximately 50%, and consumption falters ● Vasoconstriction limits the severity of hypotension
when oxygen delivery falls to around 500–600 mL/min but increases resistance to left ventricular emptying