
Page 316 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 316
12 Haematology 301
Hypersegmented
neutrophil
Macrocyte
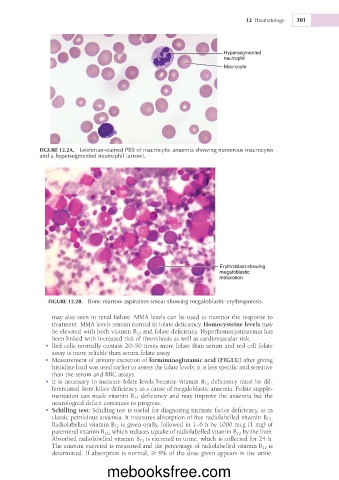
FIGURE 12.2A. Leishman-stained PBS of macrocytic anaemia showing numerous macrocytes
and a hypersegmented neutrophil (arrow).
Erythroblast showing
megaloblastic
maturation
FIGURE 12.2B. Bone marrow aspiration smear showing megaloblastic erythropoiesis.
may also seen in renal failure. MMA levels can be used to monitor the response to
treatment. MMA levels remain normal in folate deficiency. Homocysteine levels may
be elevated with both vitamin B 12 and folate deficiency. Hyperhomocystinaemia has
been linked with increased risk of thrombosis as well as cardiovascular risk.
• Red cells normally contain 20–50 times more folate than serum and red cell folate
assay is more reliable than serum folate assay.
• Measurement of urinary excretion of formiminoglutamic acid (FIGLU) after giving
histidine load was used earlier to assess the folate levels; it is less specific and sensitive
than the serum and RBC assays.
• It is necessary to measure folate levels because vitamin B 12 deficiency must be dif-
ferentiated from folate deficiency as a cause of megaloblastic anaemia. Folate supple-
mentation can mask vitamin B 12 deficiency and may improve the anaemia but the
neurological deficit continues to progress.
• Schilling test: Schilling test is useful for diagnosing intrinsic factor deficiency, as in
classic pernicious anaemia. It measures absorption of free radiolabelled vitamin B 12 .
Radiolabelled vitamin B 12 is given orally, followed in 1–6 h by 1000 mcg (1 mg) of
parenteral vitamin B 12 , which reduces uptake of radiolabelled vitamin B 12 by the liver.
Absorbed radiolabelled vitamin B 12 is excreted in urine, which is collected for 24 h.
The amount excreted is measured and the percentage of radiolabelled vitamin B 12 is
determined. If absorption is normal, 9% of the dose given appears in the urine.
mebooksfree.com