
Page 392 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 392
13 The Lung 377
4. Asbestos-related disease
(a) Prolonged exposure to asbestos dust produces three types of diseases:
(i) Asbestosis of lungs (parenchymal interstitial fibrosis)
(ii) Pleural disease (localized fibrous plaques or diffuse fibrosis)
(iii) Tumours (bronchogenic carcinoma, pleural and peritoneal mesotheliomas,
laryngeal carcinoma)
(b) Asbestos is a family of crystalline hydrated silicates that form fibres which may exist
as two distinct geometric forms:
(i) Serpentine (chrysotile): Curly and flexible fibres (90% of commercial form of
asbestos)
(ii) Amphibole: Straight, stiff and brittle fibres
(c) Amphiboles are less prevalent but more pathogenic than chrysotile as they are
more rigid and less soluble.
(d) High-risk individuals include miners, millers and fabrication workers
Pathogenesis (Flowchart 13.8):
Note: Asbestos reaches the alveoli easily, and has the ability to penetrate epithelial cells
leading to diffuse interstitial disease rather than nodular deposits as in silicosis. Asbestos
bodies are carcinogenic; can act as both initiators and promoters.
Gross pathology:
• Affected lungs are small and firm with marked thickening of the pleura.
• Variable degree of subpleural fibrosis is seen; advanced cases may show cystic
changes.
• In contrast to CWP and silicosis, asbestosis begins in the lower lobes and subpleu-
rally.
Microscopy:
• Nonspecific interstitial fibrosis with scattered asbestos bodies (asbestos fibres
coated with glycoprotein and haemosiderin, which appear as golden brown
beaded rods)
• Emphysema is seen in between areas of fibrosis.
• Pleural involvement may result in:
• Pleural effusion
• Visceral pleural fibrosis
• Pleural plaques (most common lesions with asbestos exposure; circumscribed, flat,
1 cm, firm-to-hard bilateral nodules)
Clinical features
• Slow insidious illness, which may be asymptomatic for years or may be present with
dyspnoea and dry or productive cough.
• Pulmonary hypertension and cor pulmonale are observed in advanced cases.
5. Berylliosis
(a) Due to heavy exposure to dust/fumes of metallic beryllium or its salts
(b) Used in nuclear, electronic and aerospace industries
(i) Acute berylliosis
- Seen after 2–4 weeks of exposure
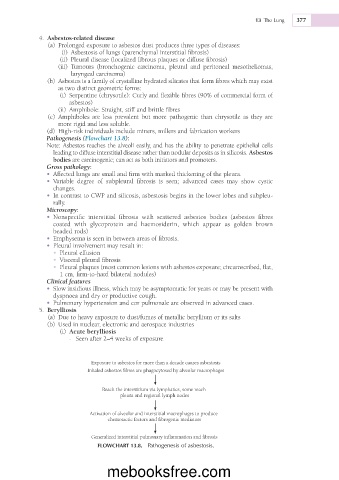
Exposure to asbestos for more than a decade causes asbestosis
Inhaled asbestos fibres are phagocytosed by alveolar macrophages
Reach the interstitium via lymphatics, some reach
pleura and regional lymph nodes
Activation of alveolar and interstitial macrophages to produce
chemotactic factors and fibrogenic mediators
Generalized interstitial pulmonary inflammation and fibrosis
FLOWCHART 13.8. Pathogenesis of asbestosis.
mebooksfree.com