
Page 532 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 532
18 Female Genital System 517
• Majority are unilateral, solid large tumours showing sheets and nests of cells with clear
cytoplasm and well-defined cytoplasmic margins, separated by thin fibrous strands.
Stroma contains lymphoid cells and may show granulomatous inflammation.
• Radio responsive with 80% survival.
(b) Teratoma: Constitutes 15–20% of ovarian tumours; more than 90% are benign mature
cystic teratomas. Other types include immature, malignant and specialized teratomas.
(i) Benign mature cystic teratomas
- Most common type is a dermoid cyst (Fig. 18.6) which is usually cystic; the
cyst is lined by stratified squamous epithelium and appendageal structures
(ectodermal differentiation) and filled with sebaceous secretion and matted hair.
- They are usually discovered accidentally on radiographs or sonograms,
picked up easily due to calcification and teeth formation.
- Ninety percent are unilateral and may present with infertility and torsion
(acute surgical emergency).
- Foci of bone and cartilage, bronchial and intestinal epithelium may some-
times be appreciated, indicating development along other germ cell layers.
- Rarely, one of the tissue elements may undergo malignant change, usually
a squamous cell carcinoma (when it is referred to as a teratoma with
malignant transformation).
(ii) Immature malignant teratomas
- Bulky, predominantly solid tumour showing foci of necrosis.
- Immature bone, cartilage, muscle, nerve and other structures are seen on
microscopy.
- Also seen are areas of neuroepithelial differentiation (lesions with such
areas tend to be aggressive and metastasize widely).
(iii) Specialized (monodermal) teratomas
Teratomas with specialized tissue, eg, struma ovarii composed entirely of
mature thyroid tissue that may hyperfunction and produce hyperthyroid-
ism or the ovarian carcinoid, which can produce carcinoid syndrome.
(c) Yolk sac (endodermal sinus) tumour of ovary
• Common in children and young adults
• Usually unilateral and presents with abdominal pain and a rapidly growing
pelvic mass
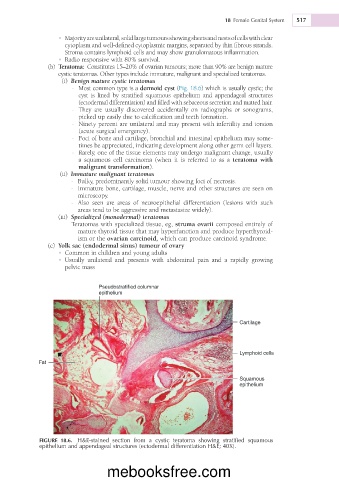
Pseudostratified columnar
epithelium
Cartilage
Lymphoid cells
Fat
Squamous
epithelium
FIGURE 18.6. H&E-stained section from a cystic teratoma showing stratified squamous
epithelium and appendageal structures (ectodermal differentiation H&E; 40X).
mebooksfree.com