
Page 1475 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1475
1310 Part VII Hematologic Malignancies
Fig. 82.1 COMPUTED TOMOGRAPHY SCAN OF THE CHEST
SHOWING A LARGE 17-CM ANTERIOR MEDIASTINAL MASS. A
biopsy was consistent with primary mediastinal B-cell lymphoma.
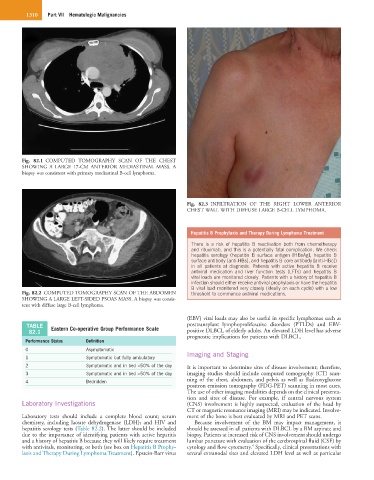
Fig. 82.3 INFILTRATION OF THE RIGHT LOWER ANTERIOR
CHEST WALL WITH DIFFUSE LARGE B-CELL LYMPHOMA.
Hepatitis B Prophylaxis and Therapy During Lymphoma Treatment
There is a risk of hepatitis B reactivation both from chemotherapy
and rituximab, and this is a potentially fatal complication. We check
hepatitis serology (hepatitis B surface antigen [HBsAg], hepatitis B
surface antibody [anti-HBs], and hepatitis B core antibody [anti-HBc])
in all patients at diagnosis. Patients with active hepatitis B receive
antiviral medication and liver function tests (LFTs) and hepatitis B
viral loads are monitored closely. Patients with a history of hepatitis B
infection should either receive antiviral prophylaxis or have the hepatitis
B viral load monitored very closely (ideally on each cycle) with a low
Fig. 82.2 COMPUTED TOMOGRAPHY SCAN OF THE ABDOMEN threshold to commence antiviral medications.
SHOWING A LARGE LEFT-SIDED PSOAS MASS. A biopsy was consis-
tent with diffuse large B-cell lymphoma.
(EBV) viral loads may also be useful in specific lymphomas such as
TABLE Eastern Co-operative Group Performance Scale posttransplant lymphoproliferative disorders (PTLDs) and EBV-
82.1 positive DLBCL of elderly adults. An elevated LDH level has adverse
prognostic implications for patients with DLBCL.
Performance Status Definition
0 Asymptomatic
1 Symptomatic but fully ambulatory Imaging and Staging
2 Symptomatic and in bed <50% of the day It is important to determine sites of disease involvement; therefore,
3 Symptomatic and in bed >50% of the day imaging studies should include computed tomography (CT) scan-
4 Bedridden ning of the chest, abdomen, and pelvis as well as fludeoxyglucose
positron emission tomography (FDG-PET) scanning in most cases.
The use of other imaging modalities depends on the clinical presenta-
tion and sites of disease. For example, if central nervous system
Laboratory Investigations (CNS) involvement is highly suspected, evaluation of the head by
CT or magnetic resonance imaging (MRI) may be indicated. Involve-
Laboratory tests should include a complete blood count; serum ment of the bone is best evaluated by MRI and PET scans.
chemistry, including lactate dehydrogenase (LDH); and HIV and Because involvement of the BM may impact management, it
hepatitis serology tests (Table 82.2). The latter should be included should be assessed in all patients with DLBCL by a BM aspirate and
due to the importance of identifying patients with active hepatitis biopsy. Patients at increased risk of CNS involvement should undergo
and a history of hepatitis B because they will likely require treatment lumbar puncture with evaluation of the cerebrospinal fluid (CSF) by
4
with antivirals, monitoring, or both (see box on Hepatitis B Prophy- cytology and flow cytometry. Specifically, clinical presentations with
laxis and Therapy During Lymphoma Treatment). Epstein-Barr virus several extranodal sites and elevated LDH level as well as particular