
Page 1478 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1478
Chapter 82 Diagnosis and Treatment of Diffuse Large B-Cell Lymphoma and Burkitt Lymphoma 1313
with favorable early stage aggressive lymphoma to receive CHOP Today, most newly diagnosed patients with DLBCL receive
alone (four cycles) or CHOP plus radiation, and found that combined rituximab in combination with a chemotherapy backbone consisting
modality therapy was not superior to chemotherapy alone. Given of cyclophosphamide, doxorubicin, vincristine, and prednisone
these results and the improved outcome of R-CHOP, it is difficult to (CHOP) (Fig. 82.5). This backbone has been used since the early
justify the routine use of radiation in early stage disease. 1970s when doxorubicin was added to cyclophosphamide, vincris-
A possible exception to the omission of radiation is in the treat- tine, and prednisone (CVP) and CHOP became the first curative
ment of primary mediastinal DLBCL (PMBL), depending on the regimen in DLBCL, highlighting the critical role of anthracyclines.
chemotherapy regimen. In a study of 50 untreated patients with Later on, in an attempt to improve upon the results with CHOP,
PMBL who received MACOP-B (methotrexate, ARA-C [Cytara- subsequent studies focused on the empiric addition of drugs to the
bine], cyclophosphamide, vincristine, prednisone, and bleomycin) regimen. However, this did not improve survival, as evidenced in a
followed by radiation, 66% had persistently positive gallium scans pivotal randomized study comparing CHOP to second and third
after chemotherapy, suggesting active disease. After consolidation generation regimens, where there was no evidence of superiority with
radiotherapy, however, only 19% of patients had a positive gallium the latter approaches, but there was much higher toxicity. Later on,
scan, and 80% were event-free at 39 months of median follow-up. other groups such as The Deutsche Studiengruppe für Hochmaligne
This important study suggested that radiotherapy was necessary after Non-Hodgkin’ Lymphome (DSHNHL) also made attempts to
chemotherapy in PMBL. Furthermore, historical evidence indicated improve the outcomes that had been observed following CHOP.
that dose-intense regimens such as MACOP-B or VACOP-B (etopo- They carried out four-arm studies of CHOP where they tested dif-
side, doxorubicin, cyclophosphamide, vincristine, prednisone, and ferent schedules of the regimen (every 14 versus every 21 days) with
bleomycin) were superior to CHOP for PMBL, raising yet another or without etoposide (CHOEP) in both older (>60 years) and
question about the optimal chemotherapy for this disease. Although younger (≤60 years) patients. While CHOEP-21 benefited patients
the addition of rituximab to CHOP has improved the outcome for
patients with DLBCL, there remains a high proportion of patients
who do not achieve remission with R-CHOP, and require mediastinal Treatment of Primary Mediastinal B-Cell Lymphoma
radiation. Recent results with the pharmacodynamically dose-adjusted
regimen of doxorubicin, vincristine, and etoposide infused over 96 Patients with a diagnosis of PMBL undergo routine CT staging of chest,
hours with bolus intravenous cyclophosphamide, rituximab, and oral abdomen, and pelvis. We administer six cycles of DA-EPOCH-R. After
prednisone (DA-EPOCH-R) challenge the need for radiation in four cycles of therapy, we repeat CT staging, and after six cycles, we
PMBL as in a prospective study of 53 patients, 93% were event-free perform CTs and an FDG-PET scan. If patients have responded and
7
with DA-EPOCH-R alone (see box on Treatment of Primary Medi- the posttherapy PET scan result is negative, we repeat CT scans every
astinal B-Cell Lymphoma). These results suggest that regimens such few months. If the FDG-PET result is positive, we attempt to perform a
as DA-EPOCH-R obviate the need for radiation in a high proportion biopsy, and if there is residual disease, patients undergo mediastinal
of patients with PMBL, thus eliminating the risk of long-term toxici- radiation treatment. If the FDG-PET result is suspicious (low SUV
values), we repeat it in 4 to 6 weeks. If at this time, the result becomes
ties such as secondary malignancies and heart disease. An ongoing negative, patients go into routine follow-up, and if it remains abnormal,
study by the International Extranodal Lymphoma Study Group we perform a biopsy and administer radiation if the biopsy confirms
(IELSG) is testing if mediastinal radiation can be omitted in patients residual disease.
who have a negative FDG-PET scan at the end of therapy. 8
Pre-Rituximab Ongoing studies
CHOP
V
m-BACOD, CHOP CHOP Improved R-CHOP-21 R-CHOP-14 R-CHOP
ProMACE- remains V outcome V not superior V
CytaBOM or standard R-CHOP with R-CHOP R-CHOP-14 DA-EPOCH-R
MACOP-B
CHOP-14, CHOEP -21 R-CHOP-14, Gains with RB-CHOP
CHOEP-14, benefits ≤ 60y R-CHOEP-14, CHOEP-21 and V
CHOP-21 or and CHOP-14 R-CHOP-21, CHOP-14 do R-CHOP
CHOEP-21 >60 y or R-CHOEP-21 not remain
with adding R
R-CHOP-I
V
R-CHOP
R-CHOP Improved
V survival with R2-CHOP
ACVBP-R (Young, ACVBP-R in V
low IPI patients) this group R-CHOP
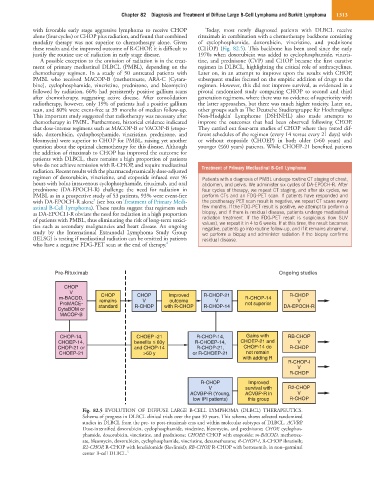
Fig. 82.5 EVOLUTION OF DIFFUSE LARGE B-CELL LYMPHOMA (DLBCL) THERAPEUTICS.
Schema of progress in DLBCL clinical trials over the past 30 years. This schema shows selected randomized
studies in DLBCL from the pre- to post-rituximab eras and within molecular subtypes of DLBCL. ACVBP,
Dose-intensified doxorubicin, cyclophosphamide, vindesine, bleomycin, and prednisone; CHOP, cyclophos-
phamide, doxorubicin, vincristine, and prednisone; CHOEP, CHOP with etoposide; m-BACOD, methotrex-
ate, bleomycin, doxorubicin, cyclophosphamide, vincristine, dexamethasone; R-CHOP-I, R-CHOP ibrutinib;
R2-CHOP, R-CHOP with lenalidomide (Revlimid); RB-CHOP, R-CHOP with bortezomib, in non–germinal
5
center B-cell DLBCL.