
Page 1798 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1798
1602 Part X Transplantation
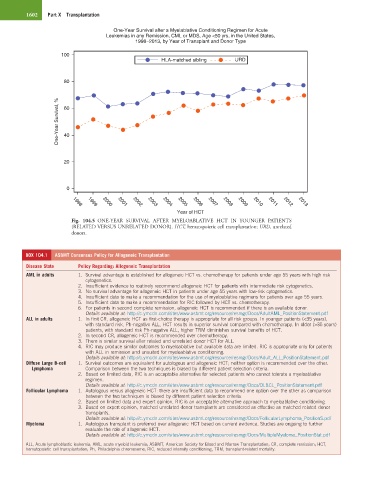
One-Year Survival after a Myelablative Conditioning Regimen for Acute
Leukemias in any Remission, CML or MDS, Age <50 yrs, in the United States,
1998−2013, by Year of Transplant and Donor Type
100
HLA-matched sibling URD
80
One-Year Survival, % 60
40
20
0
2001
2003
1998
1999
2002
2005
2006
2004
2000
Year of HCT 2007 2008 2009 2010 2011 2012 2013
Fig. 104.5 ONE-YEAR SURVIVAL AFTER MYELOABLATIVE HCT IN YOUNGER PATIENTS
(RELATED VERSUS UNRELATED DONOR). HCT, hematopoietic cell transplantation; URD, unrelated
donors.
BOX 104.1 ASBMT Consensus Policy for Allogeneic Transplantation
Disease State Policy Regarding: Allogeneic Transplantation
AML in adults 1. Survival advantage is established for allogeneic HCT vs. chemotherapy for patients under age 55 years with high risk
cytogenetics.
2. Insufficient evidence to routinely recommend allogeneic HCT for patients with intermediate risk cytogenetics.
3. No survival advantage for allogeneic HCT in patients under age 55 years with low-risk cytogenetics.
4. Insufficient data to make a recommendation for the use of myeloablative regimens for patients over age 55 years.
5. Insufficient data to make a recommendation for RIC followed by HCT vs. chemotherapy.
6. For patients in second complete remission, allogeneic HCT is recommended if there is an available donor.
Details available at: http://c.ymcdn.com/sites/www.asbmt.org/resource/resmgr/Docs/AdultAML_PositionStatement.pdf
ALL in adults 1. In first CR, allogeneic HCT as first-choice therapy is appropriate for all risk groups. In younger patients (<35 years),
with standard risk, Ph-negative ALL, HCT results in superior survival compared with chemotherapy. In older (>35 years)
patients, with standard risk Ph-negative ALL, higher TRM diminishes survival benefits of HCT.
2. In second CR, allogeneic HCT is recommended over chemotherapy.
3. There is similar survival after related and unrelated donor HCT for ALL.
4. RIC may produce similar outcomes to myeloablative but available data are limited. RIC is appropriate only for patients
with ALL in remission and unsuited for myeloablative conditioning.
Details available at: http://c.ymcdn.com/sites/www.asbmt.org/resource/resmgr/Docs/Adult_ALL_PositionStatement.pdf
Diffuse Large B-cell 1. Survival outcomes are equivalent for autologous and allogeneic HCT; neither option is recommended over the other.
Lymphoma Comparison between the two techniques is biased by different patient selection criteria.
2. Based on limited data, RIC is an acceptable alternative for selected patients who cannot tolerate a myeloablative
regimen.
Details available at: http://c.ymcdn.com/sites/www.asbmt.org/resource/resmgr/Docs/DLBCL_PositionStatement.pdf
Follicular Lymphoma 1. Autologous versus allogeneic HCT: there are insufficient data to recommend one option over the other as comparison
between the two techniques is biased by different patient selection criteria.
2. Based on limited data and expert opinion, RIC is an acceptable alternative approach to myeloablative conditioning.
3. Based on expert opinion, matched unrelated donor transplants are considered as effective as matched related donor
transplants.
Details available at: http://c.ymcdn.com/sites/www.asbmt.org/resource/resmgr/Docs/FollicularLymphoma_PositionS.pdf
Myeloma 1. Autologous transplant is preferred over allogeneic HCT based on current evidence. Studies are ongoing to further
evaluate the role of allogeneic HCT.
Details available at: http://c.ymcdn.com/sites/www.asbmt.org/resource/resmgr/Docs/MultipleMyeloma_PositionStat.pdf
ALL, Acute lymphoblastic leukemia; AML, acute myeloid leukemia; ASBMT, American Society for Blood and Marrow Transplantation; CR, complete remission; HCT,
hematopoietic cell transplantation; Ph, Philadelphia chromosome; RIC, reduced intensity conditioning, TRM, transplant-related mortality.