
Page 749 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 749
636 Part V Red Blood Cells
sufficient to cause RBC fragmentation with hemolytic anemia under
conditions of normal circulatory shear stress.
C 5 The pathobiology of the elliptocytic shape is less clear. RBC
C 5 C precursors in common HE are round and the cells become progres-
sively more elliptical as they age in vivo. RBCs subjected to shear
3 C 3 C stress in vitro, or RBCs flowing through microcirculation in vivo,
have an elliptical or parachute-like shape, respectively. It is possible
3 3 that elliptocytes and poikilocytes are permanently stabilized in their
abnormal shape because the weakened spectrin heterodimer contacts
α facilitate skeletal reorganization, which follows axial deformation of
3 3
β cells resulting from application of a prolonged or excessive shear
stress. This reorganization is likely to involve breakage of the unidi-
5 5 rectionally stretched protein connections followed by the formation
of new protein contacts that preclude the recovery of a normal
biconcave shape. This process has been shown to account for perma-
C 3 C 3 nent deformation of irreversibly sickled cells.
In HPP, the recessively inherited form of HE characterized by
severe hemolysis, RBCs have two abnormalities. They contain a
mutant spectrin that characteristically disrupts spectrin heterodimer
α β self-association, and they are also partially deficient in spectrin, as
C C evidenced by a decreased spectrin/band 3 ratio. In some HPP cases,
β α this biochemical phenotype is a consequence of a double heterozygous
state for an elliptocytogenic α-spectrin mutation and a defect involv-
ing reduced α-spectrin synthesis. Such synthetic defect of α-spectrin
Protein dysfunctions is fully asymptomatic in the heterozygous carrier, because under
HE, HPP SpD-SpD normal conditions, the synthesis of α-spectrin is approximately three
HE 4.1-SP
Spectrin to four times greater than that of β-spectrin.
Protein deficiencies: When present in conjunction with an elliptocytogenic mutation
Adducin of α-spectrin, such a synthetic defect augments the expression of the
HE 4.1 and HE 4.1°
Tropomyosin HE GPC° mutant spectrin. Because the elliptocytogenic α-spectrin mutants
C Actin are often unstable, the combination of the two defects leads to
2.1 4.1 spectrin deficiency in the cells. Other HPP patients are homozygous
or doubly heterozygous for one or two elliptocytogenic spectrin
mutations, respectively. In such cases, the spectrin deficiency may
be a consequence of spectrin instability that reduces the amount of
spectrin available for membrane assembly. Furthermore, in RBCs
containing a high fraction of unassembled dimeric spectrin, the
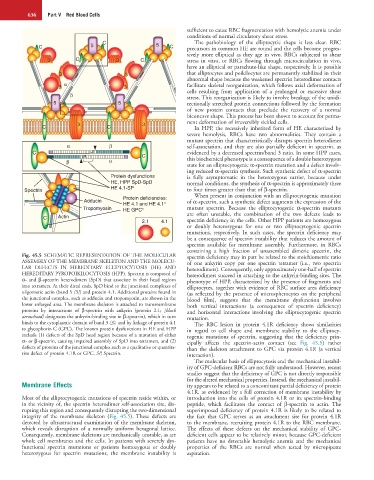
Fig. 45.5 SCHEMATIC REPRESENTATION OF THE MOLECULAR spectrin deficiency may in part be related to the stoichiometric ratio
ASSEMBLY OF THE MEMBRANE SKELETON AND THE MOLECU- of one ankyrin copy per one spectrin tetramer (i.e., two spectrin
LAR DEFECTS IN HEREDITARY ELLIPTOCYTOSIS (HE) AND heterodimers). Consequently, only approximately one-half of spectrin
HEREDITARY PYROPOIKILOCYTOSIS (HPP). Spectrin is composed of heterodimers succeed in attaching to the ankyrin-binding sites. The
α- and β-spectrin heterodimers (SpD) that associate in their head regions phenotype of HPP, characterized by the presence of fragments and
into tetramers. At their distal ends, SpD bind to the junctional complexes of elliptocytes, together with evidence of RBC surface area deficiency
oligomeric actin (band 5 [5]) and protein 4.1. Additional proteins found in (as reflected by the presence of microspherocytes on the peripheral
the junctional complex, such as adducin and tropomyosin, are shown in the blood film), suggests that the membrane dysfunction involves
lower enlarged area. The membrane skeleton is attached to transmembrane both vertical interactions (a consequence of spectrin deficiency)
proteins by interactions of β-spectrin with ankyrin (protein 2.1; [black and horizontal interactions involving the elliptocytogenic spectrin
arrowhead] designates the ankyrin-binding site in β-spectrin), which in turn mutation.
binds to the cytoplasmic domain of band 3 (3), and by linkage of protein 4.1 The RBC lesion in protein 4.1R deficiency shows similarities
to glycophorin C (GPC). The known protein dysfunctions in HE and HPP in regard to cell shape and membrane stability to the elliptocy-
include (1) defects of the SpD head region because of a mutation of either togenic mutations of spectrin, suggesting that the deficiency prin-
α- or β-spectrin, causing impaired assembly of SpD into tetramers, and (2) cipally affects the spectrin-actin contact (see Fig. 45.5) rather
defects of proteins of the junctional complex such as a qualitative or quantita- than the skeleton attachment to GPC via protein 4.1R (a vertical
tive defect of protein 4.1R or GPC. SP, Spectrin. interaction).
The molecular basis of elliptocytosis and the mechanical instabil-
ity of GPC-deficient RBCs are not fully understood. However, recent
studies suggest that the deficiency of GPC is not directly responsible
for the altered mechanical properties. Instead, the mechanical instabil-
Membrane Effects ity appears to be related to a concomitant partial deficiency of protein
4.1R, as evidenced by a full correction of membrane instability by
Most of the elliptocytogenic mutations of spectrin reside within, or introduction into the cells of protein 4.1R or its spectrin-binding
in the vicinity of, the spectrin heterodimer self-association site, dis- peptide, which facilitates the contact of β-spectrin to actin. The
rupting this region and consequently disrupting the two-dimensional superimposed deficiency of protein 4.1R is likely to be related to
integrity of the membrane skeleton (Fig. 45.5). These defects are the fact that GPC serves as an attachment site for protein 4.1R
detected by ultrastructural examination of the membrane skeleton, to the membrane, recruiting protein 4.1R to the RBC membrane.
which reveals disruption of a normally uniform hexagonal lattice. The effects of these defects on the mechanical stability of GPC-
Consequently, membrane skeletons are mechanically unstable, as are deficient cells appear to be relatively minor, because GPC-deficient
whole cell membranes and the cells. In patients with severely dys- patients have no detectable hemolytic anemia and the mechanical
functional spectrin mutations or patients homozygous or doubly properties of the RBCs are normal when tested by micropipette
heterozygous for spectrin mutations, the membrane instability is aspiration.