
Page 770 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 770
Chapter 46 Autoimmune Hemolytic Anemia 657
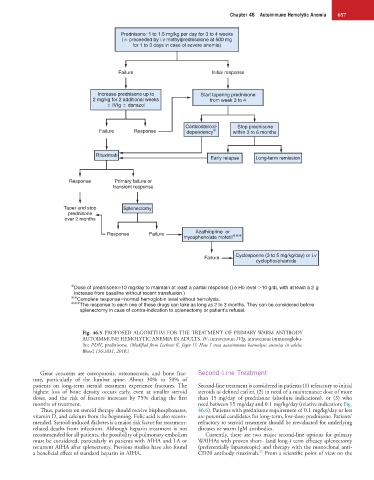
Prednisone: 1 to 1.5 mg/kg per day for 3 to 4 weeks
( preceeded by i.v methylprednisolone at 500 mg
for 1 to 3 days in case of severe anemia)
Failure Initial response
Increase prednisone up to Start tapering prednisone
2 mg/kg for 2 additional weeks from week 3 to 4
IVIg danazol
Corticosteroid- Stop prednisone
Failure Response dependency ∗ within 3 to 6 months
Rituximab
Early relapse Long-term remission
Response Primary failure or
transient response
Taper and stop Splenectomy
prednisone
over 2 months
Response Failure Azathioprine or ∗∗∗
mycophenolate mofetil
Failure Cyclosporine (3 to 5 mg/kg/day) or i.v
cyclophosphamide
∗ Dose of prednisone 10 mg day to maintain at least a partial response (i.e Hb level 10 g dL with at least a 2 g
increase from baseline without recent transfusion )
∗∗ Complete response normal hemoglobin level without hemolysis.
∗∗∗ The response to each one of these drugs can take as long as 2 to 3 months. They can be considered before
splenectomy in case of contra-indication to splenectomy or patient’s refusal.
Fig. 46.5 PROPOSED ALGORITHM FOR THE TREATMENT OF PRIMARY WARM ANTIBODY
AUTOIMMUNE HEMOLYTIC ANEMIA IN ADULTS. IV, intravenous; IVIg, intravenous immunoglobu-
lin; PDN, prednisone. (Modified from Lechner K, Jäger U: How I treat autoimmune haemolytic anemias in adults.
Blood 116:1831, 2010.)
Great concerns are osteoporosis, osteonecrosis, and bone frac- Second-Line Treatment
ture, particularly of the lumbar spine. About 30% to 50% of
patients on long-term steroid treatment experience fractures. The Second-line treatment is considered in patients (1) refractory to initial
highest loss of bone density occurs early, even at smaller steroid steroids as defined earlier, (2) in need of a maintenance dose of more
doses, and the risk of fracture increases by 75% during the first than 15 mg/day of prednisone (absolute indications), or (3) who
months of treatment. need between 15 mg/day and 0.1 mg/kg/day (relative indication; Fig.
Thus, patients on steroid therapy should receive bisphosphonates, 46.6). Patients with prednisone requirement of 0.1 mg/kg/day or less
vitamin D, and calcium from the beginning. Folic acid is also recom- are potential candidates for long-term, low-dose prednisone. Patients’
mended. Steroid-induced diabetes is a major risk factor for treatment- refractory to steroid treatment should be reevaluated for underlying
related deaths from infections. Although heparin treatment is not diseases or warm IgM antibodies.
recommended for all patients, the possibility of pulmonary embolism Currently, there are two major second-line options for primary
must be considered, particularly in patients with AIHA and LA or WAIHAs with proven short- (and long-) term efficacy splenectomy
recurrent AIHA after splenectomy. Previous studies have also found (preferentially laparoscopic) and therapy with the monoclonal anti-
35
a beneficial effect of standard heparin in AIHA. CD20 antibody rituximab. From a scientific point of view on the