
Page 1473 - Williams Hematology ( PDFDrive )
P. 1473
1448 Part X: Malignant Myeloid Diseases Chapter 89: Chronic Myelogenous Leukemia and Related Disorders 1449
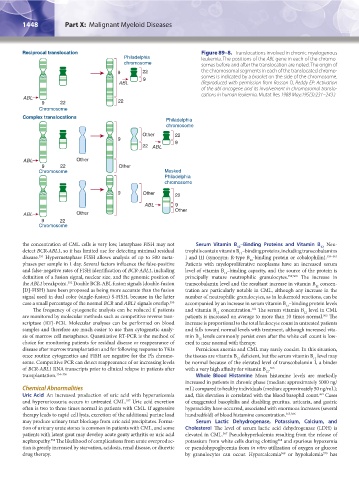
Reciprocal translocation Figure 89–8. Translocations involved in chronic myelogenous
Philadelphia leukemia. The positions of the ABL gene in each of the chromo-
chromosome somes before and after the translocation are noted. The origin of
9 22 the chromosomal segments in each of the translocated chromo-
9 somes is indicated by a bracket on the side of the chromosome.
ABL (Reproduced with permission from Rosson D, Reddy EP: Activation
of the abl oncogene and its involvement in chromosomal translo-
cations in human leukemia. Mutat Res 1988 May;195(3):231–243.)
ABL
9 22 22
Chromosome
Complex translocations
Philadelphia
chromosome
Other 22
9
9
22 ABL
ABL Other
9 22 Other
Chromosome Masked
Philadelphia
chromosome
9 Other 22
ABL 9
Other
ABL Other
9 22
Chromosome
the concentration of CML cells is very low, interphase FISH may not Serum Vitamin B –Binding Proteins and Vitamin B Neu-
12
12
detect BCR-ABL1, so it has limited use for detecting minimal residual trophils contain vitamin B –binding proteins, including transcobalamins
12
disease. Hypermetaphase FISH allows analysis of up to 500 meta- I and III (synonym: R-type B -binding protein or cobalophilin). 359–362
351
12
phases per sample in 1 day. Several factors influence the false-positive Patients with myeloproliferative neoplasms have an increased serum
and false-negative rates of FISH identification of BCR-ABL1, including level of vitamin B –binding capacity, and the source of the protein is
12
definition of a fusion signal, nuclear size, and the genomic position of principally mature neutrophilic granulocytes. 359,360 The increase in
the ABL1 breakpoint. Double BCR-ABL fusion signals (double-fusion transcobalamin level and the resultant increase in vitamin B concen-
352
12
[D]-FISH) have been proposed as being more accurate than the fusion tration are particularly notable in CML, although any increase in the
signal used in dual color (single-fusion) S-FISH, because in the latter number of neutrophilic granulocytes, as in leukemoid reactions, can be
case a small percentage of the normal BCR and ABL1 signals overlap. 353 accompanied by an increase in serum vitamin B –binding protein levels
12
The frequency of cytogenetic analysis can be reduced if patients and vitamin B concentration. The serum vitamin B level in CML
362
12
12
are monitored by molecular methods such as competitive reverse tran- patients is increased on average to more than 10 times normal. The
363
scriptase (RT)-PCR. Molecular analyses can be performed on blood increase is proportional to the total leukocyte count in untreated patients
samples and therefore are much easier to use than cytogenetic analy- and falls toward normal levels with treatment, although increased vita-
sis of marrow cell metaphases. Quantitative RT-PCR is the method of min B levels commonly persist even after the white cell count is low-
12
choice for monitoring patients for residual disease or reappearance of ered to near normal with therapy.
disease after marrow transplantation and for following response to TKIs Pernicious anemia and CML may rarely coexist. In this situation,
once routine cytogenetics and FISH are negative for the Ph chromo- the tissues are vitamin B deficient, but the serum vitamin B level may
12
12
some. Competitive PCR can detect reappearance of or increasing levels be normal because of the elevated level of transcobalamin I, a binder
of BCR-ABL1 RNA transcripts prior to clinical relapse in patients after with a very high affinity for vitamin B . 363
12
transplantation. 354–356 Whole Blood Histamine Mean histamine levels are markedly
increased in patients in chronic phase (median: approximately 5000 ng/
Chemical Abnormalities mL) compared to healthy individuals (median: approximately 50 ng/mL);
Uric Acid An increased production of uric acid with hyperuricemia and, this elevation is correlated with the blood basophil count. Cases
364
and hyperuricosuria occurs in untreated CML. Uric acid excretion of exaggerated basophilia and disabling pruritus, urticaria, and gastric
357
often is two to three times normal in patients with CML. If aggressive hyperacidity have occurred, associated with enormous increases (several
therapy leads to rapid cell lysis, excretion of the additional purine load hundredfold) of blood histamine concentration. 365,366
may produce urinary tract blockage from uric acid precipitates. Forma- Serum Lactic Dehydrogenase, Potassium, Calcium, and
tion of urinary urate stones is common in patients with CML, and some Cholesterol The level of serum lactic acid dehydrogenase (LDH) is
patients with latent gout may develop acute gouty arthritis or uric acid elevated in CML. Pseudohyperkalemia resulting from the release of
367
nephropathy. The likelihood of complications from urate overproduc- potassium from white cells during clotting and spurious hypoxemia
358
368
tion is greatly increased by starvation, acidosis, renal disease, or diuretic or pseudohypoglycemia from in vitro utilization of oxygen or glucose
drug therapy. by granulocytes can occur. Hypercalcemia or hypokalemia has
370
369
Kaushansky_chapter 89_p1437-1490.indd 1448 9/18/15 3:41 PM