
Page 1632 - Williams Hematology ( PDFDrive )
P. 1632
1606 Part XI: Malignant Lymphoid Diseases Chapter 97: Hodgkin Lymphoma 1607
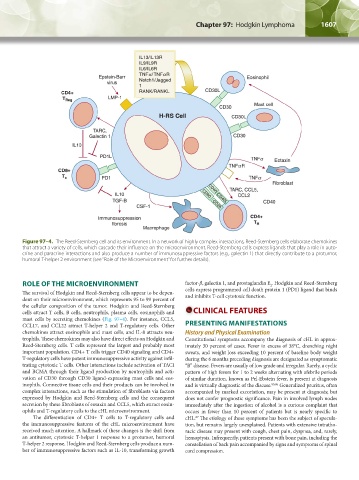
Figure 97–4. The Reed-Sternberg cell and its environment. In a network of highly complex interactions, Reed-Sternberg cells elaborate chemokines
that attract a variety of cells, which cascade their influence on the microenvironment. Reed-Sternberg cells express ligands that play a role in auto-
crine and paracrine interactions and also produce a number of immunosuppressive factors (e.g., galectin 1) that directly contribute to a protumor,
humoral T-helper 2 environment (see “Role of the Microenvironment” for further details).
ROLE OF THE MICROENVIRONMENT factor-β, galectin 1, and prostaglandin E . Hodgkin and Reed-Sternberg
2
The survival of Hodgkin and Reed-Sternberg cells appear to be depen- cells express programmed cell death protein 1 (PD1) ligand that binds
and inhibits T-cell cytotoxic function.
dent on their microenvironment, which represents 95 to 99 percent of
the cellular composition of the tumor. Hodgkin and Reed-Sternberg
cells attract T cells, B cells, neutrophils, plasma cells, eosinophils and CLINICAL FEATURES
mast cells by secreting chemokines (Fig. 97–4). For instance, CCL5,
CCL17, and CCL22 attract T-helper 2 and T-regulatory cells. Other PRESENTING MANIFESTATIONS
chemokines attract eosinophils and mast cells, and IL-8 attracts neu- History and Physical Examination
trophils. These chemokines may also have direct effects on Hodgkin and Constitutional symptoms accompany the diagnosis of cHL in approx-
Reed-Sternberg cells. T cells represent the largest and probably most imately 30 percent of cases. Fever in excess of 38°C, drenching night
important population. CD4+ T cells trigger CD40 signaling and CD4+ sweats, and weight loss exceeding 10 percent of baseline body weight
T-regulatory cells have potent immunosuppressive activity against infil- during the 6 months preceding diagnosis are designated as symptomatic
trating cytotoxic T cells. Other interactions include activation of TACI “B” disease. Fevers are usually of low grade and irregular. Rarely, a cyclic
and BCMA through their ligand production by neutrophils and acti- pattern of high fevers for 1 to 2 weeks alternating with afebrile periods
vation of CD30 through CD30 ligand-expressing mast cells and eos- of similar duration, known as Pel-Ebstein fever, is present at diagnosis
inophils. Connective tissue cells and their products can be involved in and is virtually diagnostic of the disease. 85,86 Generalized pruritus, often
complex interactions, such as the stimulation of fibroblasts via factors accompanied by marked excoriation, may be present at diagnosis; but
expressed by Hodgkin and Reed-Sternberg cells and the consequent does not confer prognostic significance. Pain in involved lymph nodes
secretion by these fibroblasts of eotaxin and CCL5, which attract eosin- immediately after the ingestion of alcohol is a curious complaint that
ophils and T-regulatory cells to the cHL microenvironment. occurs in fewer than 10 percent of patients but is nearly specific to
The differentiation of CD4+ T cells to T-regulatory cells and cHL. The etiology of these symptoms has been the subject of specula-
87
the immunosuppressive features of the cHL microenvironment have tion, but remains largely unexplained. Patients with extensive intratho-
received much attention. A hallmark of these changes is the shift from racic disease may present with cough, chest pain, dyspnea, and, rarely,
an antitumor, cytotoxic T-helper 1 response to a protumor, humoral hemoptysis. Infrequently, patients present with bone pain, including the
T-helper 2 response. Hodgkin and Reed-Sternberg cells produce a num- constellation of back pain accompanied by signs and symptoms of spinal
ber of immunosuppressive factors such as IL-10, transforming growth cord compression.
Kaushansky_chapter 97_p1603-1624.indd 1607 9/18/15 11:11 PM