
Page 1706 - Williams Hematology ( PDFDrive )
P. 1706
1680 Part XI: Malignant Lymphoid Diseases Chapter 103: Cutaneous T-Cell Lymphoma (Mycosis Fungoides and Sézary Syndrome) 1681
A B C
D E
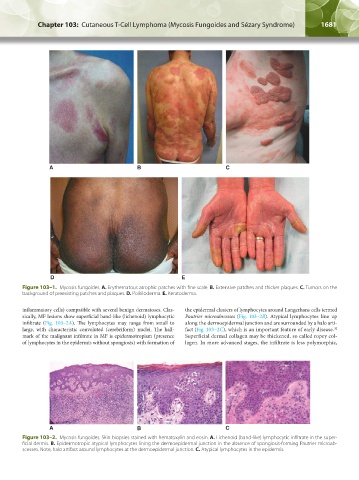
Figure 103–1. Mycosis fungoides. A. Erythematous atrophic patches with fine scale. B. Extensive patches and thicker plaques. C. Tumors on the
background of preexisting patches and plaques. D. Poikiloderma. E. Keratoderma.
inflammatory cells) compatible with several benign dermatoses. Clas- the epidermal clusters of lymphocytes around Langerhans cells termed
sically, MF lesions show superficial band-like (lichenoid) lymphocytic Pautrier microabscesses (Fig. 103–2B). Atypical lymphocytes line up
infiltrate (Fig. 103–2A). The lymphocytes may range from small to along the dermoepidermal junction and are surrounded by a halo arti-
large, with characteristic convoluted (cerebriform) nuclei. The hall- fact (Fig. 103–2C), which is an important feature of early disease.
32
mark of the malignant infiltrate in MF is epidermotropism (presence Superficial dermal collagen may be thickened, so called ropey col-
of lymphocytes in the epidermis without spongiosis) with formation of lagen. In more advanced stages, the infiltrate is less polymorphic,
A B C
Figure 103–2. Mycosis fungoides. Skin biopsies stained with hematoxylin and eosin. A. Lichenoid (band-like) lymphocytic infiltrate in the super-
ficial dermis. B. Epidermotropic atypical lymphocytes lining the dermoepidermal junction in the absence of spongiosis-forming Pautrier microab-
scesses. Note, halo artifact around lymphocytes at the dermoepidermal junction. C. Atypical lymphocytes in the epidermis.
Kaushansky_chapter 103_p1679-1692.indd 1681 9/21/15 12:50 PM