
Page 2251 - Williams Hematology ( PDFDrive )
P. 2251
2226 Part XII: Hemostasis and Thrombosis Chapter 130: Hereditary Thrombophilia 2227
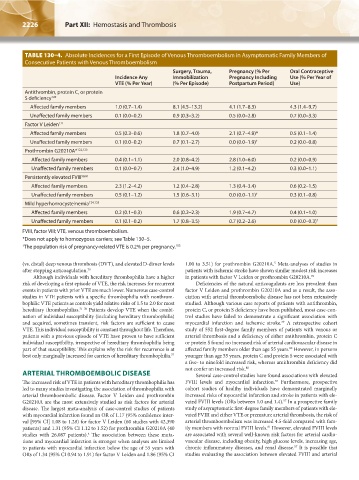
TABLE 130–4. Absolute Incidences for a First Episode of Venous Thromboembolism in Asymptomatic Family Members of
Consecutive Patients with Venous Thromboembolism
Surgery, Trauma, Pregnancy (% Per Oral Contraceptive
Incidence Any Immobilization Pregnancy Including Use (% Per Year of
VTE (% Per Year) (% Per Episode) Postpartum Period) Use)
Antithrombin, protein C, or protein
S deficiency 120
Affected family members 1.0 (0.7–1.4) 8.1 (4.5–13.2) 4.1 (1.7–8.3) 4.3 (1.4–9.7)
Unaffected family members 0.1 (0.0–0.2) 0.9 (0.3–3.2) 0.5 (0.0–2.8) 0.7 (0.0–3.3)
Factor V Leiden 121
Affected family members 0.5 (0.3–0.6) 1.8 (0.7–4.0) 2.1 (0.7–4.9)* 0.5 (0.1–1.4)
Unaffected family members 0.1 (0.0–0.2) 0.7 (0.1–2.7) 0.0 (0.0–1.9) † 0.2 (0.0–0.8)
Prothrombin G20210A* 122,123
Affected family members 0.4 (0.1–1.1) 2.0 (0.8–4.2) 2.8 (1.0–6.0) 0.2 (0.0–0.9)
Unaffected family members 0.1 (0.0–0.7) 2.4 (1.0–4.9) 1.2 (0.1–4.2) 0.3 (0.0–1.1)
Persistently elevated FVIII 58,81
Affected family members 2.3 (1.2–4.2) 1.2 (0.4–2.8) 1.3 (0.4–3.4) 0.6 (0.2–1.5)
Unaffected family members 0.5 (0.1–1.2) 1.5 (0.6–3.1) 0.0 (0.0–1.1) † 0.3 (0.1–0.8)
Mild hyperhomocysteinemia 124,125
Affected family members 0.2 (0.1–0.3) 0.6 (0.2–2.3) 1.9 (0.7–4.7) 0.4 (0.1–1.0)
Unaffected family members 0.1 (0.1–0.2) 1.7 (0.8–3.5) 0.7 (0.2–2.6) 0.0 (0.0–0.3) †
FVIII, factor VIII; VTE, venous thromboembolism.
*Does not apply to homozygous carriers; see Table 130–5.
† The population risk of pregnancy-related VTE is 0.2% per pregnancy. 103
(vs. distal) deep venous thrombosis (DVT), and elevated D-dimer levels 1.00 to 3.51) for prothrombin G20210A. Meta-analyses of studies in
5
after stopping anticoagulation. 70 patients with ischemic stroke have shown similar modest risk increases
Although individuals with hereditary thrombophilia have a higher in patients with factor V Leiden or prothrombin G20210A. 78
risk of developing a first episode of VTE, the risk increases for recurrent Deficiencies of the natural anticoagulants are less prevalent than
events in patients with prior VTE are much lower. Numerous case-control factor V Leiden and prothrombin G20210A and as a result, the asso-
studies in VTE patients with a specific thrombophilia with nonthrom- ciation with arterial thromboembolic disease has not been extensively
bophilic VTE patients as controls yield relative risks of 1.5 to 2.0 for most studied. Although various case reports of patients with antithrombin,
hereditary thrombophilias. 71–76 Patients develop VTE when the combi- protein C, or protein S deficiency have been published, most case-con-
nation of individual susceptibility (including hereditary thrombophilia) trol studies have failed to demonstrate a significant association with
and acquired, sometimes transient, risk factors are sufficient to cause myocardial infarction and ischemic stroke. A retrospective cohort
79
VTE. This individual susceptibility is constant throughout life. Therefore, study of 552 first-degree family members of patients with venous or
patients with a previous episode of VTE have proven to have sufficient arterial thrombosis and a deficiency of either antithrombin, protein C
individual susceptibility, irrespective of hereditary thrombophilia being or protein S found no increased risk of arterial cardiovascular disease in
part of that susceptibility. This explains why the risk for recurrence is at affected family members older than age 55 years. However, in persons
80
best only marginally increased for carriers of hereditary thrombophilia. 77 younger than age 55 years, protein C and protein S were associated with
a five- to ninefold increased risk, whereas antithrombin deficiency did
not confer an increased risk. 80
ARTERIAL THROMBOEMBOLIC DISEASE Several case-control studies have found associations with elevated
The increased risk of VTE in patients with hereditary thrombophilia has FVIII levels and myocardial infarction. Furthermore, prospective
57
led to many studies investigating the association of thrombophilia with cohort studies of healthy individuals have demonstrated marginally
arterial thromboembolic disease. Factor V Leiden and prothrombin increased risks of myocardial infarction and stroke in patients with ele-
G20210A are the most extensively studied as risk factors for arterial vated FVIII levels (ORs between 1.0 and 1.4). In a prospective family
57
disease. The largest meta-analysis of case-control studies of patients study of asymptomatic first-degree family members of patients with ele-
with myocardial infarction found an OR of 1.17 (95% confidence inter- vated FVIII and either VTE or premature arterial thrombosis, the risk of
val [95% CI] 1.08 to 1.28) for factor V Leiden (60 studies with 42,390 arterial thromboembolism was increased 4.5-fold compared with fam-
patients) and 1.31 (95% CI 1.12 to 1.52) for prothrombin G20210A (40 ily members with normal FVIII levels. However, elevated FVIII levels
81
studies with 26,087 patients). The association between these muta- are associated with several well-known risk factors for arterial cardio-
4
tions and myocardial infarction is stronger when analyses are limited vascular disease, including obesity, high glucose levels, increasing age,
57
to patients with myocardial infarction below the age of 55 years with chronic inflammatory diseases, and renal disease. It is possible that
ORs of 1.34 (95% CI 0.94 to 1.91) for factor V Leiden and 1.86 (95% CI studies evaluating the association between elevated FVIII and arterial
Kaushansky_chapter 130_p2221-2232.indd 2226 9/21/15 4:33 PM