
Page 905 - Williams Hematology ( PDFDrive )
P. 905
880 Part VI: The Erythrocyte Chapter 57: Primary and Secondary Erythrocytoses 881
Hgb Hct CLINICAL FEATURES
(gm %) (%)
20 PRIMARY POLYCYTHEMIA
60 Primary Familial and Congenital Polycythemia
Although PFCP is uncommon, it is frequently misdiagnosed. Unlike
18
15 50 patients with polycythemia vera, patients with PFCP lack splenomegaly,
neutrophilia, basophilia, thrombocytosis, and a JAK2 mutation. Unless
exposed to alkylating agents or radioactive phosphorus, as many have
40
been, these patients do not progress to acute leukemia or myelodysplas-
159
10 tic syndrome. Generally thought to be benign, this condition predis-
30
Hct Hgb poses patients to severe cardiovascular problems because of chronic
augmented erythropoietin signaling in all tissues bearing EPOR.
160
20 An increased incidence of cardiovascular disease has been observed
161
5 in affected members of PFCP families. Erythrocytosis may be very
10 severe, with hemoglobin levels that typically exceed 20 g/dL in men and
18 g/dL in women. Headaches are commonly present. Hypertension,
coronary artery disease, and strokes have been reported, but do not
0 0 clearly appear to be related to an elevated hematocrit as they also occur
Methyl testosterone
100 in aggressively phlebotomized patients with normal hematocrits, and
162
mg/day 0 are not a constant feature of the disorder. 163
50 Fluoxymesterone
0 Chuvash Polycythemia
The recessive polycythemia that is endemic in the Chuvash Autono-
Months 0 2 4 6 8 10 12 14 16 18
mous Republic of the Russian Federation is characterized by elevation
of the hemoglobin level to a mean of 22.6 with a standard deviation of
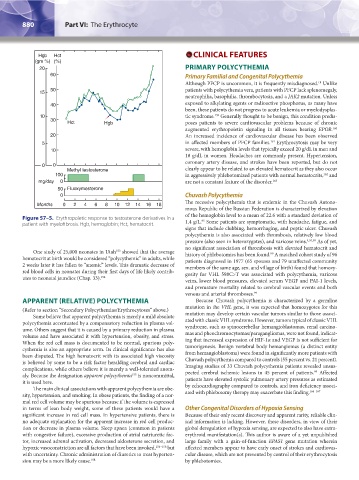
Figure 57–5. Erythropoietic response to testosterone derivatives in a 1.4 g/L. Some patients are symptomatic, with headache, fatigue, and
95
patient with myelofibrosis. Hgb, hemoglobin; Hct, hematocrit.
signs that include clubbing, hemorrhaging, and peptic ulcer. Chuvash
polycythemia is also associated with thrombosis, relatively low blood
pressure (also seen in heterozygotes), and varicose veins. 4,95,99 As of yet,
no significant association of thrombosis with elevated hematocrit and
One study of 25,000 neonates in Utah showed that the average history of phlebotomies has been found. A matched cohort study of 96
153
99
hematocrit at birth would be considered “polycythemic” in adults, while patients diagnosed in 1977 (65 spouses and 79 unaffected community
2 weeks later it has fallen to “anemic” levels. This dramatic decrease of members of the same age, sex, and village of birth) found that homozy-
red blood cells in neonates during their first days of life likely contrib- gosity for VHL 598C>T was associated with polycythemia, varicose
utes to neonatal jaundice (Chap. 33). 154 veins, lower blood pressures, elevated serum VEGF and PAI-1 levels,
and premature mortality related to cerebral vascular events and both
venous and arterial thromboses. 99
APPARENT (RELATIVE) POLYCYTHEMIA Because Chuvash polycythemia is characterized by a germline
(Refer to section “Secondary Polycythemias/Erythrocytoses” above.) mutation in the VHL gene, it was expected that homozygotes for this
Some believe that apparent polycythemia is merely a mild absolute mutation may develop certain vascular tumors similar to those associ-
polycythemia accentuated by a compensatory reduction in plasma vol- ated with classic VHL syndrome. However, tumors typical of classic VHL
ume. Others suggest that it is caused by a primary reduction in plasma syndrome, such as spinocerebellar hemangioblastomas, renal carcino-
volume and have associated it with hypertension, obesity, and stress. mas and pheochromocytomas/paragangliomas, were not found, indicat-
When the red cell mass is documented to be normal, spurious poly- ing that increased expression of HIF-1α and VEGF is not sufficient for
cythemia is also an appropriate term. Its clinical significance has also tumorigenesis. Benign vertebral body hemangiomas (a distinct entity
been disputed. The high hematocrit with its associated high viscosity from hemangioblastoma) were found in significantly more patients with
is believed by some to be a risk factor heralding cerebral and cardiac Chuvash polycythemia compared to controls (55 percent vs. 21 percent).
complications, while others believe it is merely a well-tolerated anom- Imaging studies of 33 Chuvash polycythemia patients revealed unsus-
99
aly. Because the designation apparent polycythemia is noncommittal, pected cerebral ischemic lesions in 45 percent of patients. Affected
155
it is used here. patients have elevated systolic pulmonary artery pressures as estimated
The main clinical associations with apparent polycythemia are obe- by echocardiography compared to controls, and iron deficiency associ-
164–167
sity, hypertension, and smoking. In obese patients, the finding of a nor- ated with phlebotomy therapy may exacerbate this finding.
mal red cell volume may be spurious because if the volume is expressed
in terms of lean body weight, some of these patients would have a Other Congenital Disorders of Hypoxia Sensing
significant increase in red cell mass. In hypertensive patients, there is Because of their only recent discovery and apparent rarity, reliable clin-
no adequate explanation for the apparent increase in red cell produc- ical information is lacking. However, these disorders, in view of their
tion or decrease in plasma volume. Sleep apnea (common in patients global deregulation of hypoxia sensing, are expected to also have extra-
with congestive failure), excessive production of atrial natriuretic fac- erythroid manifestation(s). This author is aware of a yet unpublished
tor, increased adrenal activation, decreased aldosterone secretion, and large family with a gain-of-function EPAS1 gene mutation wherein
hypoxic vasoconstriction are all factors that have been invoked, 156–158 but affected members appear to have early onset of strokes and cardiovas-
with uncertainty. Chronic administration of diuretics to treat hyperten- cular disease, which are not prevented by control of their erythrocytosis
sion may be a more likely cause. 158 by phlebotomies.
Kaushansky_chapter 57_p0871-0888.indd 880 9/18/15 9:36 AM