
Page 472 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 472
CHaPTEr 32 Approach to the Evaluation of the Patient With Suspected Immunodeficiency 453
TABLE 32.1 Clinical Clues of Significance for the Diagnosis of Immunodeficiencies
T-Cell Function antibody Granulocyte
Defect Defect Defects Complement Defect IFN-γ/IL-12 Defect
Recurrent or severe bacterial infections X X X (catalase-positive) X (encapsulated bacteria)
Systemic mycobacterial infections X X
Recurrent or severe viral infections X X X X
Invasive fungal infections X X
Opportunistic infections X X X
Failure to thrive X X X
Autoimmunity X X X X
Lymphoma X X (CVID)
CVID, common variable immunodeficiency; IFN, interferon; IL, interleukin.
TABLE 32.2 Nonimmunological Clinical
Findings Present in Immunodeficiency
Syndromes
Nonimmunological
Clinical Finding Immunodeficiency
Small platelets, thrombocytopenia, Wiskott-Aldrich syndrome (WAS)
eczema
Conical teeth, ectodermal Nuclear factor κB (NF-κB)
dysplasia essential modulator (NEMO)
defect
Delayed shedding of primary Autosomal dominant hyper-IgE
teeth, frequent fractures, syndrome (AD-HIES)
hyperextensibility
Cerebellar ataxia, telangiectasia Ataxia–telangiectasia (AT)
Hypoparathyroidism, conotruncal DiGeorge syndrome
heart defect, velopalatal
insufficiency
Short limbs Cartilage-hair hypoplasia
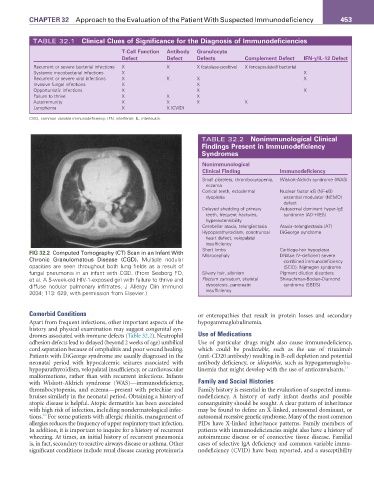
FIG 32.2 Computed Tomography (CT) Scan in an Infant With Microcephaly DNAse IV–deficient severe
Chronic Granulomatous Disease (CGD). Multiple nodular combined immunodeficiency
opacities are seen throughout both lung fields as a result of (SCID), Nijmegen syndrome
fungal pneumonia in an infant with CGD. (From Seeborg FO, Silvery hair, albinism Pigment dilution disorders
et al. A 5-week-old HIV-1-exposed girl with failure to thrive and Pectum carinatum, skeletal Shwachman-Bodian-Diamond
diffuse nodular pulmonary infiltrates. J Allergy Clin Immunol dysostosis, pancreatic syndrome (SBDS)
2004; 113: 629, with permission from Elsevier.) insufficiency
Comorbid Conditions or enteropathies that result in protein losses and secondary
Apart from frequent infections, other important aspects of the hypogammaglobulinemia.
history and physical examination may suggest congenital syn-
dromes associated with immune defects (Table 32.2). Neutrophil Use of Medications
adhesion defects lead to delayed (beyond 2 weeks of age) umbilical Use of particular drugs might also cause immunodeficiency,
cord separation because of omphalitis and poor wound healing. which could be predictable, such as the use of rituximab
Patients with DiGeorge syndrome are usually diagnosed in the (anti-CD20 antibody) resulting in B-cell depletion and potential
neonatal period with hypocalcemic seizures associated with antibody deficiency, or idiopathic, such as hypogammaglobu-
hypoparathyroidism, velopalatal insufficiency, or cardiovascular linemia that might develop with the use of anticonvulsants. 11
malformations, rather than with recurrent infections. Infants
with Wiskott-Aldrich syndrome (WAS)—immunodeficiency, Family and Social Histories
thrombocytopenia, and eczema—present with petechiae and Family history is essential in the evaluation of suspected immu-
bruises similarly in the neonatal period. Obtaining a history of nodeficiency. A history of early infant deaths and possible
atopic disease is helpful. Atopic dermatitis has been associated consanguinity should be sought. A clear pattern of inheritance
with high risk of infection, including nondermatological infec- may be found to define an X-linked, autosomal dominant, or
10
tions. For some patients with allergic rhinitis, management of autosomal recessive genetic syndrome. Many of the most common
allergies reduces the frequency of upper respiratory tract infection. PIDs have X-linked inheritance patterns. Family members of
In addition, it is important to inquire for a history of recurrent patients with immunodeficiencies might also have a history of
wheezing. At times, an initial history of recurrent pneumonia autoimmune disease or of connective tissue disease. Familial
is, in fact, secondary to reactive airways disease or asthma. Other cases of selective IgA deficiency and common variable immu-
significant conditions include renal disease causing proteinuria nodeficiency (CVID) have been reported, and a susceptibility